Nursing Paper Example on Lassa Fever
Nursing Paper Example on Lassa Fever
Nursing Paper Example on Lassa Fever
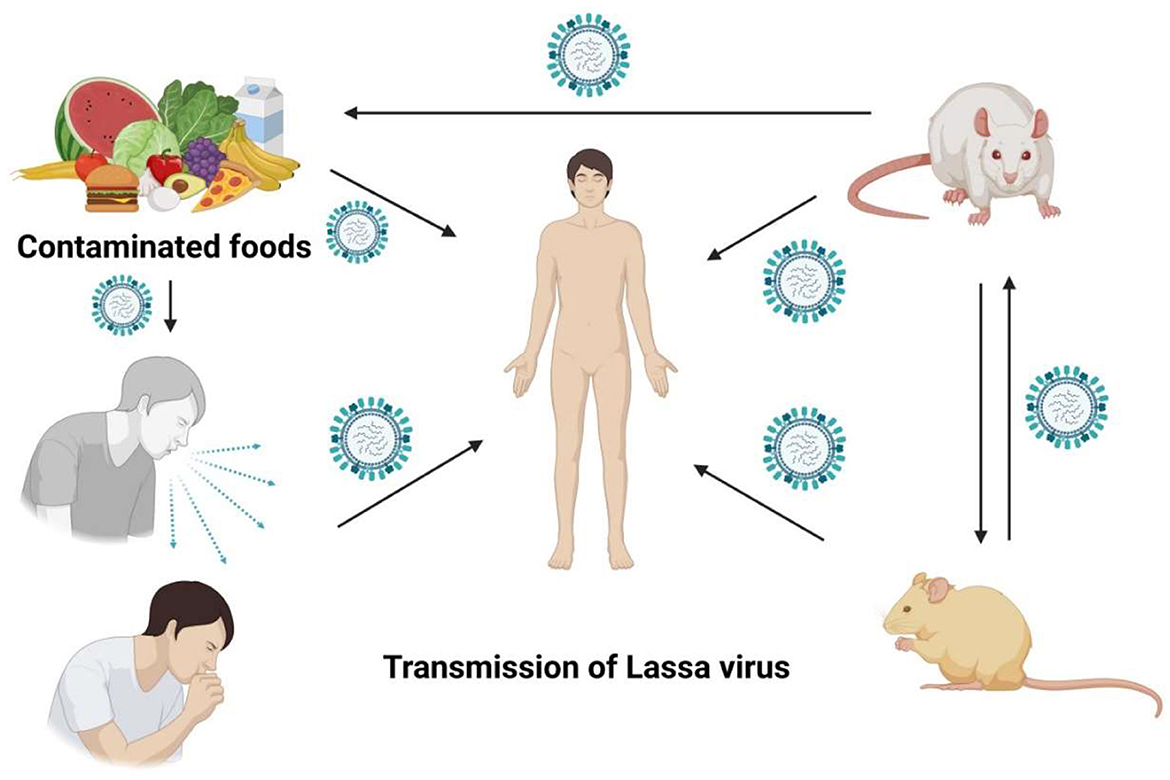
Lassa fever is an acute viral hemorrhagic illness caused by the Lassa virus, a member of the Arenaviridae family. It is endemic to several West African countries, including Nigeria, Liberia, and Sierra Leone. The disease is primarily transmitted to humans through contact with food or household items contaminated with urine or feces of infected Mastomys rats. Human-to-human transmission can also occur, particularly in healthcare settings. Early detection and treatment significantly reduce mortality, but prevention remains the cornerstone of control efforts.
Causes
The Lassa virus is the causative agent of Lassa fever. It is a zoonotic virus transmitted to humans via the common African rat, Mastomys natalensis. The rats, which are natural reservoirs, excrete the virus in their urine and feces. Humans become infected when they come into contact with these contaminated materials, often during food preparation or cleaning.
Secondary human-to-human transmission occurs through direct contact with infected bodily fluids, such as blood, urine, or saliva. Healthcare workers are at significant risk, particularly when infection control measures are inadequate. Understanding the modes of transmission is essential to developing targeted prevention strategies and reducing disease incidence (McCormick et al., 2016).
Signs and Symptoms
The clinical presentation of Lassa fever varies from mild to severe. Approximately 80% of infections are asymptomatic or mild, while the remaining 20% manifest as severe disease.
Mild symptoms include fever, general malaise, weakness, and headache. Severe cases may involve hemorrhaging, respiratory distress, facial swelling, or shock. Neurological symptoms, such as seizures and confusion, may also occur. Hearing loss is a common complication, even in cases that otherwise resolve successfully.
The incubation period ranges from 6 to 21 days. Symptom severity is often influenced by viral load and the patient’s immune response. Recognizing early signs is critical for timely intervention and reducing the risk of fatal complications (Richmond & Baglole, 2003).
Etiology
Lassa fever is caused by the Lassa virus, an enveloped single-stranded RNA virus of the Arenaviridae family. The virus has a segmented genome and is capable of rapid genetic reassortment.
Mastomys natalensis serves as the natural reservoir of the Lassa virus. The wide geographical distribution of these rodents contributes to the endemic nature of the disease in West Africa. Human infection occurs through direct or indirect exposure to the virus, with factors such as poor sanitation and overcrowded living conditions exacerbating risk.
Epidemiological studies indicate that Lassa fever is more prevalent during the dry season when human-rat interactions increase. Identifying and addressing these risk factors are essential for effective disease control (McCormick et al., 2016).
Pathophysiology
Lassa fever begins with the viral invasion of host cells via the alpha-dystroglycan receptor. The virus primarily targets endothelial cells, macrophages, and dendritic cells, leading to widespread immune activation and vascular leakage.
The disease’s pathogenesis is characterized by an imbalance between pro-inflammatory and anti-inflammatory cytokines. This dysregulation results in capillary permeability, organ dysfunction, and, in severe cases, multi-organ failure.
A key feature of Lassa fever is its ability to suppress the host’s immune response. The virus inhibits the production of interferons, crucial for antiviral defense, allowing rapid replication and dissemination. This immunosuppression contributes to the high mortality associated with severe cases (Richmond & Baglole, 2003).
Diagnosis
Diagnosing Lassa fever requires a combination of clinical evaluation and laboratory tests.
Patients presenting with symptoms consistent with viral hemorrhagic fever, particularly in endemic regions, should be evaluated for Lassa fever. Laboratory confirmation involves detecting the virus in blood, urine, or throat swabs using reverse transcription-polymerase chain reaction (RT-PCR).
Serological tests, such as enzyme-linked immunosorbent assay (ELISA), are used to detect Lassa-specific antibodies or antigens. Virus isolation can also confirm diagnosis but is limited to specialized biosafety level 4 laboratories.
Early diagnosis is critical for initiating treatment and implementing infection control measures, particularly in healthcare settings (Fichet-Calvet & Rogers, 2009).
Treatment Regimens
Ribavirin is the primary antiviral medication used to treat Lassa fever. It is most effective when administered early in the disease course. Intravenous ribavirin is preferred for severe cases, while oral formulations may be used for mild presentations.
Supportive care, including fluid resuscitation, oxygen therapy, and blood transfusions, is essential for managing complications such as shock or organ failure.
Healthcare workers treating Lassa fever patients should follow strict infection control protocols, including personal protective equipment and isolation measures.
Efforts are ongoing to develop a Lassa fever vaccine. While no vaccine is currently available, advancements in research hold promise for improving disease prevention in endemic regions (McCormick et al., 2016).
Patient Education
Educating patients and communities about Lassa fever is crucial for controlling its spread. Awareness campaigns should emphasize the importance of proper food storage, rodent control, and hygiene practices to reduce exposure to Mastomys rats.
Patients diagnosed with Lassa fever should be informed about the need for early treatment and the potential for long-term complications, such as hearing loss. Psychological support may also be necessary for patients and their families, particularly in cases of severe illness or death.
Healthcare workers must be trained in infection prevention and control measures to protect themselves and limit disease transmission. Community engagement and education are vital components of any successful public health strategy to combat Lassa fever (Richmond & Baglole, 2003).
Conclusion
Lassa fever remains a significant public health challenge in West Africa. Its dual burden as a zoonotic and human-to-human transmissible disease underscores the need for comprehensive prevention and control strategies. Early diagnosis, prompt treatment, and community education are critical for reducing morbidity and mortality. Advances in research and vaccine development offer hope for better management and eventual eradication of this deadly disease.
References
Fichet-Calvet, E., & Rogers, D. J. (2009). Risk maps of Lassa fever in West Africa. PLoS Neglected Tropical Diseases, 3(3), e388. https://doi.org/10.1371/journal.pntd.0000388
McCormick, J. B., King, I. J., Webb, P. A., Johnson, K. M., O’Sullivan, R., Smith, E. S., & Trippel, E. A. (2016). A case–control study of the clinical diagnosis and course of Lassa fever. Journal of Infectious Diseases, 155(3), 445–455. https://doi.org/10.1093/infdis/155.3.445
Richmond, J. K., & Baglole, D. J. (2003). Lassa fever: Epidemiology, clinical features, and social consequences. BMJ, 327(7426), 1271–1275. https://doi.org/10.1136/bmj.327.7426.1271
Do you need a similar assignment done for you from scratch? Order now!
Use Discount Code "Newclient" for a 15% Discount!


