
Blog
Pitocin Side Effects: A Comprehensive Guide for Nursing Students (Assessment, Complications, and Nursing Management)
Pitocin Side Effects Explained: A Comprehensive Guide to Oxytocin, Labor Induction, Intravenous Pitocin Administration, Risks of Pitocin, and Pitocin and Birth Injuries
Introduction
Pitocin side effects are among the most important medication safety considerations in modern obstetric care because Pitocin directly influences the physiology of labor and has the potential to affect both maternal and fetal outcomes. As a synthetic form of oxytocin, Pitocin is used extensively to induce labor, augment labor, and manage specific obstetric conditions when the benefits of delivery outweigh the risks of continuing the pregnancy. While the medication has significantly improved the management of labor and delivery, its effectiveness depends on appropriate patient selection, careful dose titration, vigilant monitoring, and prompt recognition of adverse effects. Even small changes in the dose of Pitocin can alter the pattern and strength of uterine contractions, making a thorough understanding of Pitocin side effects essential for safe clinical practice.
The administration of Pitocin is not simply the initiation of an intravenous infusion. Rather, it is a dynamic clinical process that requires continuous assessment of maternal and fetal responses throughout labor. Unlike many medications that produce predictable therapeutic effects, Pitocin influences several physiologic systems simultaneously. As oxytocin stimulates the smooth muscle of the uterus, it increases the frequency, duration, and intensity of each uterine contraction. These changes are intended to promote cervical dilation and facilitate vaginal birth, but excessive stimulation may compromise uteroplacental blood flow, reduce oxygen delivery to the fetus, and increase the risk of obstetric emergencies.
Understanding Pitocin side effects begins with appreciating the delicate balance between therapeutic benefit and potential harm. The desired outcome of Pitocin administration is effective labor progression through coordinated uterine activity. However, because the medication acts directly on oxytocin receptors within the myometrium, excessive uterine stimulation can occur if the medication is not carefully titrated. This explains why Pitocin is classified as a high-alert medication in many healthcare institutions and why standardized administration protocols have become an integral component of obstetric safety initiatives.
Several factors influence how an individual responds to Pitocin, making every labor unique. These include:
- Maternal age and overall health.
- Gestational age.
- Cervical readiness before labor induction.
- Previous uterine surgery or cesarean delivery.
- Fetal position and presentation.
- Individual sensitivity to synthetic oxytocin.
- Existing maternal or fetal medical conditions.
Because these variables differ among patients, no single infusion rate or dosing schedule is appropriate for every clinical situation. Instead, the administration of Pitocin requires individualized assessment and frequent adjustments based on maternal and fetal responses rather than predetermined timelines.
Although Pitocin has become one of the most commonly used for labor induction, its use is associated with both expected physiologic responses and potential complications. Common side effects are generally mild and manageable with appropriate monitoring, whereas more serious complications may develop rapidly if excessive uterine activity is not recognized early. Potential adverse outcomes include:
- Uterine tachysystole and hyperstimulation.
- Abnormal fetal heart rate patterns.
- Fetal distress resulting from decreased placental perfusion.
- Maternal hypotension or fluid-related complications.
- Postpartum hemorrhage.
- Rare but life-threatening complications such as uterine rupture.
- Severe Pitocin and birth injuries resulting from prolonged fetal oxygen deprivation.
These complications illustrate why the effects of Pitocin extend beyond the uterus alone. Changes in uterine activity directly influence placental circulation, fetal oxygenation, maternal hemodynamics, and ultimately the safety of both the mother and baby throughout childbirth.
Safe Pitocin use therefore depends on more than understanding the medication’s pharmacology. It requires integrating clinical assessment with evidence-based decision-making throughout labor. Healthcare providers must continuously evaluate:
- Whether labor is progressing appropriately.
- The quality, frequency, and duration of each contraction.
- Maternal vital signs and overall clinical status.
- Continuous fetal heart rate monitoring.
- Signs of excessive uterine activity or compromised fetal oxygenation.
- Whether the Pitocin infusion should be maintained, reduced, temporarily discontinued, or stopped altogether.
These ongoing assessments allow clinicians to identify evolving complications before they progress into preventable maternal or neonatal emergencies.
The decision to use Pitocin to induce labor is likewise based on careful clinical evaluation rather than convenience. In many pregnancies, women enter spontaneous labor without pharmacologic intervention. In others, however, medical conditions such as post-term pregnancy, hypertensive disorders, ruptured membranes without adequate contractions, or maternal illnesses necessitate labor induction to improve outcomes. In cases where the cervix is not yet favorable, cervical ripening agents such as Cervidil may be administered before initiating Pitocin, highlighting the importance of understanding both Pitocin and Cervidil within the broader context of induction management.
In addition to clinical knowledge, modern obstetric practice emphasizes medication safety and risk reduction. Recommendations from the Food and Drug Administration, the Institute for Safe Medication Practices, and professional obstetric organizations underscore the importance of standardized infusion protocols, independent medication verification, continuous electronic fetal monitoring when indicated, accurate documentation, and prompt interdisciplinary communication. These evidence-based practices are designed to minimize the risks associated with Pitocin while preserving its considerable benefits in appropriately selected patients.
This article provides a comprehensive examination of Pitocin side effects, beginning with the pharmacology of oxytocin, the clinical indications and contraindications for Pitocin induction, and the principles of safe intravenous Pitocin administration. It then explores maternal and fetal adverse effects, serious complications including Pitocin and birth injuries, evidence-based nursing assessment and management strategies, current safety recommendations, and important legal considerations related to Pitocin use. By understanding both the therapeutic actions and the potential side effects of Pitocin, healthcare professionals can contribute to safer labor and delivery, improve maternal and neonatal outcomes, and promote evidence-based care throughout the childbirth process.
Understanding Pitocin and Oxytocin
Understanding the relationship between Pitocin and oxytocin forms the foundation for recognizing Pitocin side effects, appreciating its therapeutic benefits, and safely managing patients during labor and delivery. Before administering the medication or monitoring for adverse reactions, healthcare professionals should understand how Pitocin is a synthetic medication designed to mimic the actions of a naturally occurring hormone, how it affects the uterus, and why it is prescribed in specific obstetric situations. A clear understanding of these principles also explains why the administration of Pitocin requires careful monitoring and why inappropriate Pitocin use may result in serious maternal and fetal complications.
What Pitocin Is and How Oxytocin Works
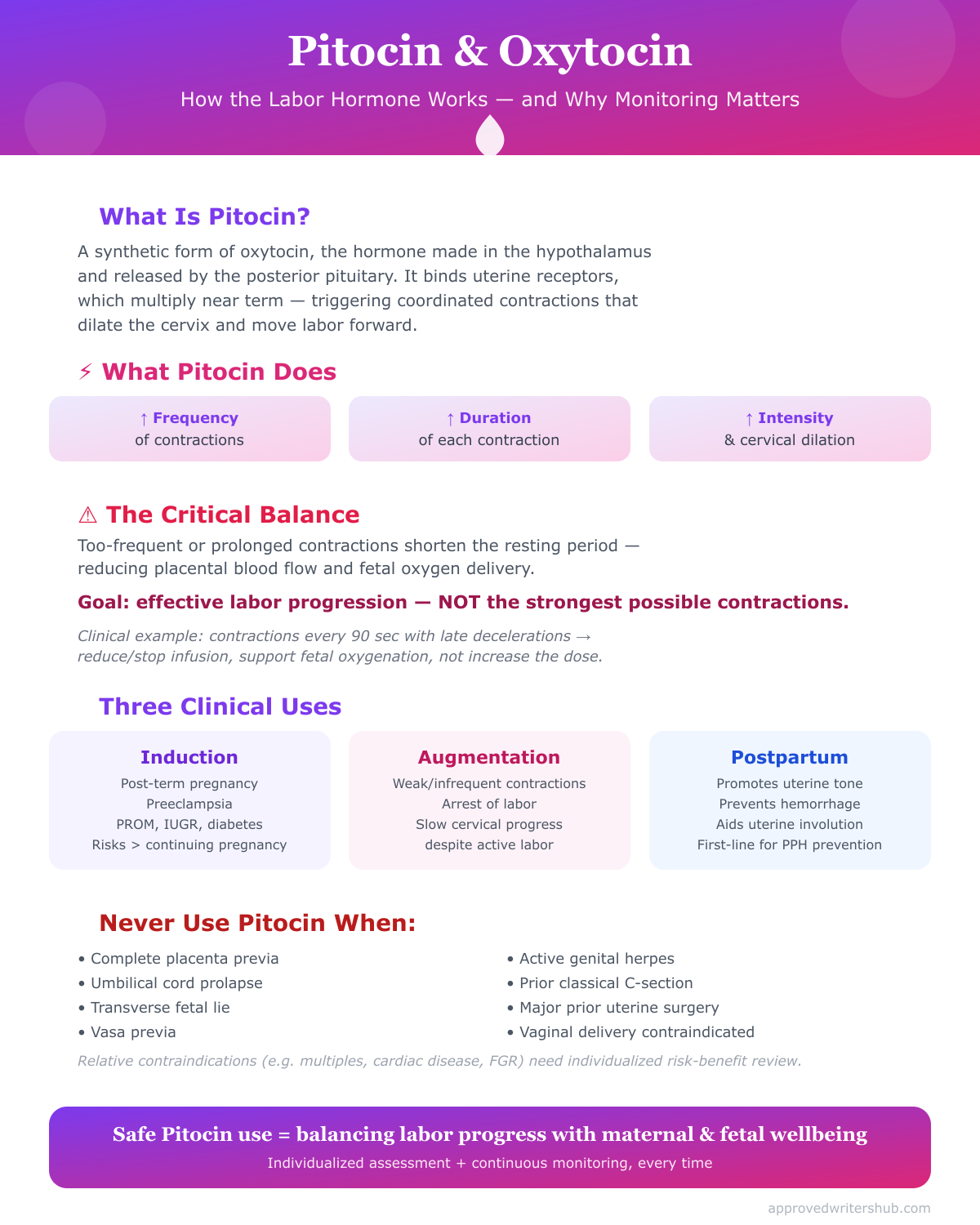
Oxytocin is a hormone naturally synthesized in the hypothalamus and released by the posterior pituitary gland. It plays a central role throughout pregnancy, childbirth, and the postpartum period by regulating uterine activity and facilitating maternal adaptation after delivery. Although oxytocin is produced continuously in small amounts, its secretion increases significantly near term, contributing to the onset of labor through coordinated uterine contractions.
Pitocin is the pharmaceutical or synthetic form of oxytocin developed to replicate the physiologic actions of the naturally occurring hormone. Because it has the same biologic activity as endogenous oxytocin, Pitocin is used to stimulate uterine contractions when spontaneous labor is absent, delayed, or progressing inadequately. Once administered intravenously, the medication circulates rapidly and binds to specific oxytocin receptors located within the smooth muscle cells of the uterus.
The number of oxytocin receptors present in the uterus is not constant throughout pregnancy. Instead, receptor density increases dramatically during the final weeks of gestation, making the uterus progressively more responsive to both endogenous oxytocin and synthetic oxytocin. This physiologic adaptation explains why Pitocin to induce labor is generally effective only after the pregnancy has reached an appropriate gestational age.
After binding to uterine receptors, Pitocin stimulates a series of intracellular events that increase calcium availability within uterine muscle cells. Elevated intracellular calcium promotes contraction of myometrial fibers, resulting in coordinated and rhythmic uterine contractions that gradually dilate the cervix and facilitate fetal descent through the birth canal.
The physiologic actions of Pitocin include:
- Increasing the frequency of uterine contractions.
- Increasing the duration of each contraction.
- Increasing contraction intensity.
- Promoting progressive cervical dilation.
- Supporting fetal descent during labor.
- Enhancing the effectiveness of labor when spontaneous contractions are inadequate.
These effects explain why Pitocin has become one of the most frequently used for labor induction worldwide.
How Oxytocin Influences Maternal and Fetal Physiology
Although the primary target of Pitocin is the uterus, its physiologic effects extend beyond uterine muscle.
During normal labor, each uterine contraction temporarily compresses maternal blood vessels supplying the placenta. Between contractions, uteroplacental blood flow returns, allowing oxygen and nutrients to reach the fetus. Under normal circumstances, this alternating pattern is well tolerated because contractions occur at appropriate intervals.
When Pitocin produces contractions that are excessively frequent or prolonged, however, the resting period between contractions becomes shorter. As a result:
- Placental blood flow decreases.
- Fetal oxygen delivery is reduced.
- Carbon dioxide removal from the fetus becomes less efficient.
- The likelihood of fetal distress increases.
- Abnormal fetal heart rate patterns may develop.
For this reason, the therapeutic goal of Pitocin administration is not to create the strongest possible contractions but rather to establish an effective contraction pattern that promotes labor progression while preserving adequate fetal oxygenation.
Another important physiologic consideration is that oxytocin possesses mild antidiuretic properties because of its structural similarity to vasopressin. When high doses of Pitocin are administered over prolonged periods, particularly with large volumes of electrolyte-free intravenous fluids, patients may develop water intoxication and dilutional hyponatremia. Although uncommon with modern infusion protocols, this complication illustrates that the effects of oxytocin extend beyond uterine activity alone.
Clinical Example
A woman undergoing labor using Pitocin develops contractions every 90 seconds, each lasting approximately 100 seconds. Continuous electronic monitoring demonstrates recurrent late decelerations in the fetal heart rate. Although labor appears to be progressing rapidly, these findings indicate excessive uterine stimulation that is compromising placental blood flow. In this situation, the priority is not to continue increasing the dose of Pitocin, but to reduce or discontinue the infusion while initiating interventions to improve fetal oxygenation.
This example demonstrates that effective labor is defined by adequate uterine activity balanced with maternal and fetal safety—not simply by stronger contractions.
Clinical Uses of Pitocin for Labor Induction
The use of Pitocin is based on the principle that the benefits of delivery should outweigh the risks of continuing the pregnancy. Healthcare providers prescribe Pitocin only after carefully evaluating maternal health, fetal condition, gestational age, cervical readiness, and the anticipated risks and benefits of intervention.
The medication is primarily used to induce labor or augment labor, although it also has important postpartum applications.
Labor induction
Pitocin induction refers to initiating labor in a woman who has not entered spontaneous labor.
Common indications include:
- Post-term pregnancy.
- Premature rupture of membranes without adequate contractions.
- Gestational hypertension.
- Preeclampsia.
- Maternal diabetes requiring delivery.
- Intrauterine growth restriction.
- Oligohydramnios.
- Certain fetal conditions in which delivery is safer than remaining in utero.
- Other situations in which the risks of continuing the pregnancy exceed the benefits of expectant management.
In these circumstances, clinicians may use Pitocin to induce labor after confirming that no contraindications exist.
Labor augmentation
Not all women receiving Pitocin require induction. Some enter spontaneous labor but experience inadequate uterine activity that prevents normal cervical dilation.
Examples include:
- Weak contractions.
- Infrequent contractions.
- Arrest of labor despite ruptured membranes.
- Slow cervical progression despite active labor.
In these situations, clinicians may administer Pitocin to stimulate contractions and improve labor efficiency while carefully monitoring maternal and fetal responses.
Postpartum management
Although commonly associated with labor induction, Pitocin also plays a major role after delivery.
Following placental delivery, Pitocin is given to:
- Promote uterine contraction.
- Reduce postpartum blood loss.
- Prevent postpartum hemorrhage.
- Improve uterine tone.
- Facilitate uterine involution.
These actions make oxytocin one of the first-line medications for preventing excessive postpartum bleeding.
Why Cervical Assessment Matters
Before initiating Pitocin, clinicians assess cervical readiness using tools such as the Bishop Score.
A favorable cervix generally demonstrates:
- Cervical dilation.
- Cervical effacement.
- Soft consistency.
- Anterior position.
- Appropriate fetal station.
When the cervix remains unfavorable, cervical ripening may be necessary before induction. In these situations, providers frequently administer prostaglandins such as Cervidil, explaining why Pitocin and Cervidil are often discussed together in obstetric practice.
Contraindications to Pitocin Use
Although Pitocin is highly effective when appropriately indicated, it should never be administered simply because labor has not yet begun. Every decision to begin Pitocin administration requires careful evaluation of maternal and fetal safety.
Certain clinical conditions make Pitocin use inappropriate because stimulation of uterine contractions could significantly increase the likelihood of maternal injury, fetal compromise, or both.
Major contraindications include:
Absolute contraindications
- Complete placenta previa.
- Umbilical cord prolapse.
- Transverse fetal lie.
- Vasa previa.
- Active genital herpes infection.
- Previous classical cesarean incision.
- Previous extensive uterine surgery involving the upper uterine segment.
- Situations in which vaginal delivery is contraindicated.
In these circumstances, attempting to induce labor with Pitocin may expose the patient to severe complications, including catastrophic hemorrhage or uterine rupture.
Relative contraindications
Certain conditions require individualized risk-benefit assessment rather than absolute avoidance.
Examples include:
- Grand multiparity.
- Multiple gestation.
- Previous low-transverse cesarean delivery.
- Maternal cardiac disease.
- Fetal growth restriction.
- Polyhydramnios.
- Suspected fetal compromise.
In these cases, clinicians carefully weigh the benefits of delivery against the risks associated with Pitocin, often opting for lower starting doses, slower titration, and more intensive maternal and fetal surveillance.
Importance of Individualized Clinical Decision-Making
No two pregnancies are identical. Decisions regarding Pitocin administration should consider the complete clinical picture rather than relying solely on a single diagnosis or protocol. Before initiating a Pitocin infusion, healthcare providers evaluate maternal history, fetal well-being, cervical status, gestational age, and the likelihood of achieving a safe vaginal birth.
A thoughtful, evidence-based approach to Pitocin use helps maximize the benefits of labor induction while minimizing Pitocin side effects, reducing the risk of complications such as fetal distress, hyperstimulation, uterine rupture, and postpartum hemorrhage, and ultimately promoting safer outcomes for both baby and the mother.
Pitocin Administration During Labor
The administration of Pitocin during labor is a carefully controlled clinical process that requires continuous assessment, individualized dosing, and close maternal and fetal monitoring. Although Pitocin is a synthetic form of oxytocin, it is not administered in the same way as most medications. Instead of prescribing a fixed dose, healthcare providers administer Pitocin intravenously using standardized infusion protocols that allow gradual dose adjustments based on the patient’s response. This individualized approach is necessary because women respond differently to synthetic oxytocin, and excessive stimulation of the uterus can quickly lead to significant Pitocin side effects.
The primary goal of Pitocin administration is to establish an effective pattern of uterine contractions that promotes cervical dilation, fetal descent, and successful vaginal delivery without compromising maternal or fetal well-being. Ideally, contractions should be regular, moderate to strong in intensity, and separated by adequate resting periods that allow the uterus to relax and restore placental blood flow to the fetus.
Healthcare providers continually balance two important objectives during labor using Pitocin:
- Achieving sufficient uterine activity to facilitate labor progression.
- Preventing excessive uterine stimulation that may result in Pitocin side effects, fetal distress, or maternal complications.
This balance explains why the medication is regarded as a high-alert medication in obstetric practice. Small increases in the infusion rate can substantially alter contraction frequency and intensity, making continuous assessment essential throughout labor and delivery.
Several factors influence how a patient responds to Pitocin, including:
- Gestational age.
- Cervical readiness.
- Number of previous pregnancies.
- Maternal sensitivity to oxytocin.
- Fetal position and presentation.
- Maternal medical conditions.
- Previous uterine surgery.
- Whether labor is being induced or augmented.
For this reason, healthcare providers should never assume that two patients will require identical dosing or respond similarly to the same infusion rate.
Intravenous Pitocin Administration and Dosage Principles
The administration of Pitocin is performed exclusively by the intravenous route during labor induction and labor augmentation because intravenous delivery allows rapid dose adjustments and immediate discontinuation if complications occur. Since Pitocin side effects can develop quickly when uterine activity becomes excessive, the ability to titrate or stop the medication promptly is a major safety advantage over other routes of administration.
Preparation of the Pitocin infusion
Before initiating therapy, the prescribed amount of Pitocin is diluted in a compatible intravenous solution according to institutional policy. The infusion is then administered using an electronic infusion pump, which delivers precise amounts of medication and minimizes dosing errors. Manual gravity infusions should never be used because they cannot provide the level of accuracy required for this high-alert medication.
To further enhance patient safety:
- Pitocin infusion should be connected as close as possible to the intravenous insertion site.
- A dedicated infusion line is preferred whenever possible.
- The infusion pump should have dose limits and safety alerts if available.
- Medication verification by two qualified clinicians is commonly recommended before initiation.
Dosage principles
There is no universal dose of Pitocin that is appropriate for every patient. Instead, the infusion is individualized according to maternal and fetal responses.
General principles include:
- Starting with a low initial infusion rate.
- Increasing the infusion gradually at predetermined intervals.
- Allowing sufficient time for each dose adjustment to produce its physiologic effect before making additional increases.
- Using the lowest effective dose necessary to achieve adequate labor.
The philosophy behind modern Pitocin induction protocols is straightforward: administer the minimum amount of medication required to produce effective labor while minimizing the likelihood of Pitocin side effects.
The desired contraction pattern generally consists of:
- Regular uterine contractions.
- Approximately three to five contractions within a 10-minute period.
- Contractions lasting about 40 to 90 seconds.
- Adequate resting time between contractions.
- Progressive cervical dilation and fetal descent.
Once this pattern has been established, additional increases in the dose of Pitocin are usually unnecessary unless labor progress slows.
Clinical example
A woman undergoing Pitocin induction begins with a low-dose infusion because she has reached 41 weeks of gestation without entering spontaneous labor. After several hours, her contractions become regular, occurring every three minutes, and cervical dilation progresses steadily from 3 cm to 6 cm. Since labor is progressing appropriately, increasing the infusion further would provide little additional benefit while increasing the risk of Pitocin side effects, including hyperstimulation and fetal distress. Maintaining the effective dose is therefore the safest approach.
Pitocin Induction Protocols and Safe Titration
Modern Pitocin induction protocols are designed to maximize therapeutic effectiveness while reducing the risks associated with Pitocin. Although specific protocols differ slightly among institutions, they share several evidence-based principles that emphasize patient safety and individualized care.
Stepwise dose titration
Safe titration involves making gradual changes in the infusion rate based on continuous clinical assessment rather than predetermined time intervals alone.
Dose adjustments should always consider:
- Frequency of uterine contractions.
- Duration of each contraction.
- Intensity of contractions.
- Resting uterine tone.
- Maternal vital signs.
- Cervical progress.
- Continuous fetal heart rate monitoring.
Rather than attempting to achieve the fastest possible labor, clinicians focus on establishing an effective contraction pattern that allows adequate placental perfusion between contractions.
Continuous maternal assessment
During Pitocin administration, maternal assessment includes:
- Blood pressure.
- Heart rate.
- Respiratory status.
- Pain level.
- Uterine activity.
- Fluid balance.
- Signs of water intoxication during prolonged infusions.
- Overall labor progression.
Any unexpected maternal symptoms may indicate developing Pitocin side effects that require immediate reassessment.
Continuous fetal assessment
Equally important is evaluation of fetal well-being.
Continuous monitoring includes assessment of:
- Baseline fetal heart rate.
- Variability.
- Accelerations.
- Decelerations.
- Overall fetal response to contractions.
Abnormal fetal heart rate patterns may indicate reduced placental blood flow caused by excessive uterine activity.
Recognizing excessive uterine activity
One of the most significant Pitocin side effects is excessive uterine stimulation.
Warning signs include:
- More than five contractions within 10 minutes.
- Contractions lasting longer than two minutes.
- Minimal relaxation between contractions.
- Elevated resting uterine tone.
- Persistent fetal heart rate abnormalities.
- Clinical evidence of fetal distress.
When these findings occur, healthcare providers should promptly reduce or discontinue the Pitocin infusion while implementing appropriate intrauterine resuscitation measures.
Why slow titration improves safety
Gradual dose adjustments allow clinicians to observe the physiologic response before administering additional medication.
This approach helps reduce the likelihood of:
- Hyperstimulation.
- Decreased placental perfusion.
- Maternal hypotension.
- Abnormal fetal heart rate patterns.
- Emergency operative delivery.
- Severe Pitocin and birth injuries.
Safe titration reflects the principle that more medication does not necessarily produce better outcomes. Instead, carefully controlled dosing promotes effective labor while preserving maternal and fetal safety.
Pitocin and Cervidil: Combined Use in Labor Induction
Successful labor induction often depends on both cervical readiness and effective uterine contractions. While Pitocin primarily stimulates uterine muscle, it has relatively little effect on cervical ripening. Consequently, some patients require cervical preparation before Pitocin administration can achieve optimal results.
One of the most commonly used cervical ripening agents is Cervidil (dinoprostone), a prostaglandin preparation that softens, effaces, and dilates the cervical tissue before active induction begins.
Differences between Pitocin and Cervidil
Although both medications are used during labor induction, they serve distinct purposes.
Pitocin primarily:
- Stimulates uterine contractions.
- Promotes labor progression.
- Augments inadequate labor.
- Helps achieve vaginal birth when medically appropriate.
Cervidil primarily:
- Softens the cervix.
- Promotes cervical effacement.
- Facilitates cervical dilation.
- Improves the likelihood of successful induction.
Rather than competing therapies, Pitocin and Cervidil are complementary medications that address different aspects of the labor process.
Sequential use during labor induction
In many induction protocols, women with an unfavorable cervix receive Cervidil before beginning Pitocin.
A typical sequence includes:
- Assessment of cervical readiness using the Bishop Score.
- Administration of Cervidil when the cervix is unfavorable.
- Observation for cervical ripening and spontaneous contractions.
- Removal of Cervidil at the appropriate time.
- Reassessment of maternal and fetal status.
- Initiation of Pitocin infusion if labor has not progressed adequately.
This staged approach often improves induction success while reducing the amount of Pitocin required to establish effective labor.
Safety considerations when combining Pitocin and Cervidil
Because both medications influence the labor process, careful timing is essential. Administering Pitocin too soon after prostaglandin therapy may increase uterine sensitivity to oxytocin, thereby raising the risk of Pitocin side effects, particularly hyperstimulation, excessive uterine contractions, and fetal distress.
For this reason, clinicians follow established waiting periods after Cervidil removal before initiating Pitocin administration, allowing the effects of the prostaglandin to diminish. Throughout this transition, continuous monitoring of maternal status, contraction patterns, and fetal heart rate remains essential.
When appropriate patient selection, standardized protocols, and careful monitoring are combined, the sequential use of Pitocin and Cervidil can improve the effectiveness of labor induction while maintaining the safety of both the mother and fetus. However, because both medications have the potential to increase uterine activity, meticulous assessment and timely intervention remain the cornerstone of preventing Pitocin side effects and achieving favorable maternal and neonatal outcomes.
Common Side Effects of Pitocin
Although Pitocin is an essential medication in modern obstetric practice, its administration is not without risk. Pitocin side effects range from mild, expected physiologic responses to severe complications that require immediate intervention. Most adverse effects occur because Pitocin stimulates the smooth muscle of the uterus, increasing the frequency, duration, and intensity of uterine contractions. While these contractions are intended to facilitate labor induction and vaginal delivery, excessive uterine activity may compromise maternal health, reduce placental blood flow, and negatively affect the fetus.
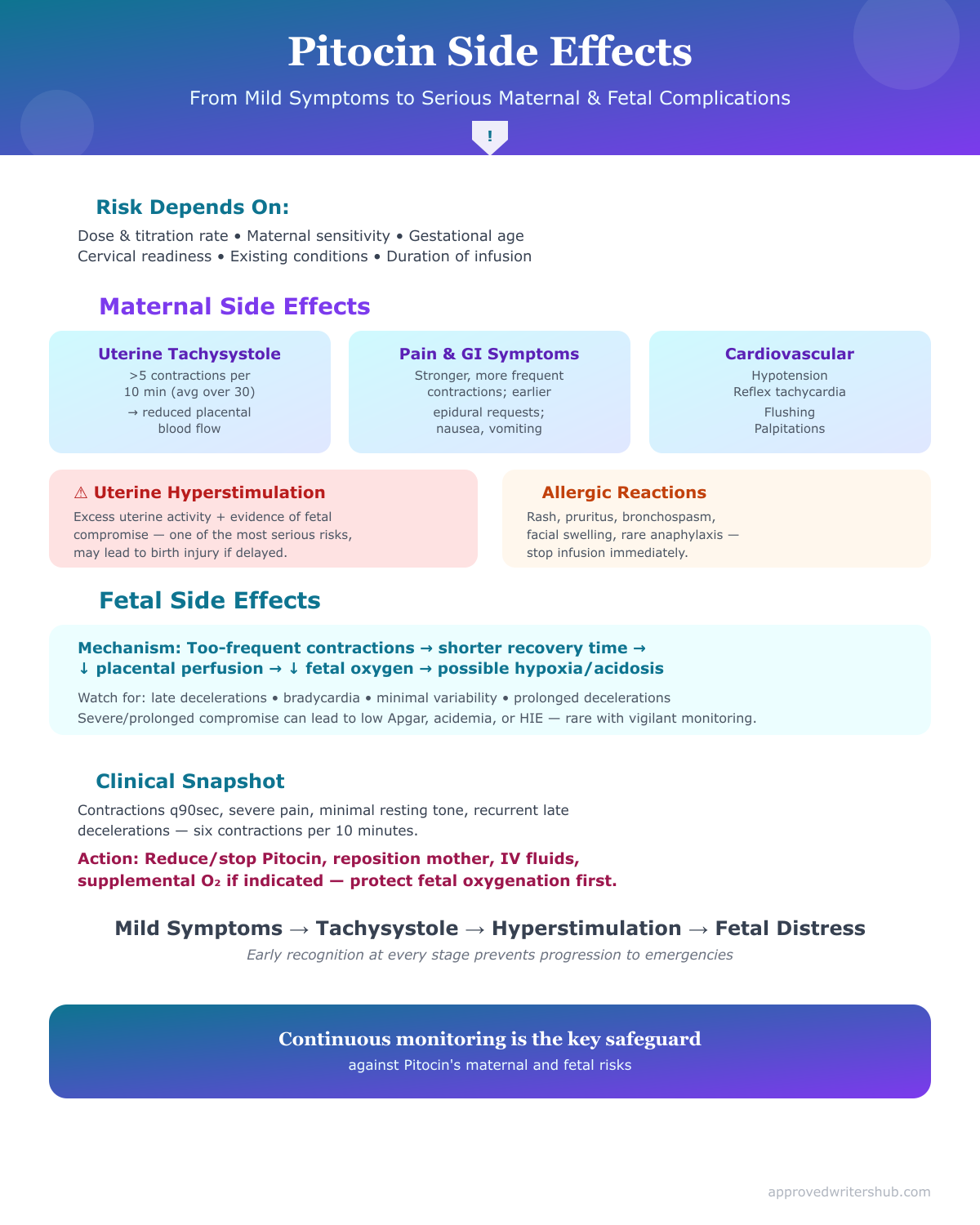
The likelihood of developing Pitocin side effects depends on several factors, including:
- The dose of Pitocin administered.
- The rate at which the medication is titrated.
- Maternal sensitivity to synthetic oxytocin.
- Gestational age.
- Cervical readiness.
- Existing maternal or fetal conditions.
- Whether Pitocin is being used to induce labor or augment labor.
- The duration of the Pitocin infusion.
Importantly, not every patient experiences adverse effects. Many women who take Pitocin progress through labor without complications when the medication is administered appropriately and monitored carefully. Nevertheless, healthcare professionals must remain vigilant because Pitocin side effects can develop rapidly and may progress from mild symptoms to life-threatening emergencies if not recognized promptly.
From a clinical perspective, the effects of Pitocin can be broadly categorized into:
- Maternal side effects.
- Fetal side effects.
- Fluid-related and systemic adverse reactions.
- Serious obstetric complications associated with excessive uterine stimulation.
Understanding each category allows healthcare providers to identify complications early and implement timely interventions that protect both mother and baby.
Maternal Side Effects of Pitocin
Maternal Pitocin side effects range from expected physiologic responses during labor to uncommon but potentially serious complications affecting multiple organ systems. Many of these adverse effects are dose-dependent, meaning they become more likely as the dose of Pitocin or duration of administration increases.
Uterine tachysystole
The most common clinically significant Pitocin side effect is uterine tachysystole.
Uterine tachysystole refers to:
- More than five uterine contractions within a 10-minute period (averaged over 30 minutes).
Excessive contraction frequency limits uterine relaxation between contractions, reducing placental blood flow and increasing the risk of fetal distress.
Clinical manifestations include:
- Very frequent contractions.
- Minimal resting time between contractions.
- Increased maternal discomfort.
- Progressive fetal heart rate abnormalities.
Because uterine tachysystole may quickly progress to hyperstimulation, continuous monitoring is essential during Pitocin administration.
Excessive labor pain
Since Pitocin stimulates stronger and more frequent contractions than those occurring during many cases of spontaneous labor, women often report greater pain intensity.
Contributing factors include:
- Increased contraction strength.
- Shorter intervals between contractions.
- Longer contraction duration.
Consequently, women receiving Pitocin infusion may request analgesia or epidural anesthesia earlier than women experiencing spontaneous labor.
Gastrointestinal symptoms
Several gastrointestinal symptoms are considered relatively common Pitocin side effects, including:
- Nausea.
- Vomiting.
- Abdominal discomfort.
Although usually mild, these symptoms may contribute to dehydration and maternal fatigue during prolonged labor using Pitocin.
Cardiovascular effects
Because oxytocin is a hormone that can influence vascular smooth muscle, cardiovascular effects may occasionally occur.
Potential manifestations include:
- Hypotension.
- Reflex tachycardia.
- Flushing.
- Palpitations.
Rapid intravenous administration or excessively concentrated infusions increase the likelihood of these complications.
Healthcare providers should monitor maternal:
- Blood pressure.
- Heart rate.
- Overall hemodynamic stability.
particularly after significant dose adjustments.
Uterine hyperstimulation
Although closely related to tachysystole, hyperstimulation represents a more severe clinical condition.
Hyperstimulation involves excessive uterine activity accompanied by evidence of fetal compromise.
This may include:
- Persistent uterine contraction.
- Inadequate uterine relaxation.
- Abnormal fetal heart rate patterns.
- Reduced placental perfusion.
Hyperstimulation represents one of the most serious Pitocin side effects because prolonged oxygen deprivation may contribute to Pitocin and birth injuries if intervention is delayed.
Allergic and hypersensitivity reactions
Although uncommon, allergic reactions to Pitocin have been reported.
Possible symptoms include:
- Rash.
- Pruritus.
- Bronchospasm.
- Facial swelling.
- Anaphylaxis (rare).
Immediate discontinuation of the medication and emergency management are required if severe hypersensitivity develops.
Clinical example
A 28-year-old woman undergoing Pitocin induction develops contractions every 90 seconds after several dose increases. She reports severe pain, increasing pelvic pressure, and difficulty recovering between contractions. Continuous monitoring demonstrates minimal resting uterine tone.
These findings suggest excessive uterine stimulation rather than normal labor progression. Prompt reduction or discontinuation of the Pitocin infusion helps prevent progression to fetal distress and other serious Pitocin side effects.
Fetal Effects of Pitocin
While many discussions focus primarily on maternal complications, Pitocin side effects can significantly affect the fetus because fetal oxygenation depends entirely on adequate uteroplacental circulation.
During each uterine contraction, blood vessels supplying the placenta are temporarily compressed. Normally, adequate relaxation between contractions restores placental blood flow, allowing oxygen exchange to resume.
When contractions become excessively frequent or prolonged because Pitocin stimulates the uterus too aggressively, this recovery period becomes inadequate.
As a result:
- Placental perfusion decreases.
- Fetal oxygen delivery declines.
- Carbon dioxide removal slows.
- Progressive hypoxia may develop.
Fetal distress
One of the most important fetal Pitocin side effects is fetal distress.
Although the term encompasses several clinical findings, it generally indicates that the fetus is not tolerating labor adequately.
Common causes include:
- Excessive uterine contractions.
- Reduced placental blood flow.
- Umbilical cord compression.
- Maternal hypotension.
Signs of fetal distress may include:
- Persistent late decelerations.
- Bradycardia.
- Minimal or absent heart rate variability.
- Prolonged decelerations.
Recognition of these findings requires immediate reassessment of the Pitocin infusion and implementation of corrective measures.
Abnormal fetal heart rate patterns
Continuous electronic monitoring allows clinicians to identify changes in the fetal heart rate before permanent injury occurs.
Potential abnormalities include:
- Recurrent late decelerations.
- Variable decelerations.
- Prolonged decelerations.
- Fetal bradycardia.
- Reduced baseline variability.
These patterns frequently represent early indicators of compromised fetal oxygenation.
Reduced fetal oxygenation
The principal mechanism underlying many fetal Pitocin side effects is diminished oxygen delivery.
When contractions occur too frequently:
- Placental blood flow decreases.
- Oxygen transfer declines.
- Metabolic acidosis may develop if hypoxia persists.
- Emergency delivery may become necessary.
Neonatal complications
Severe or prolonged fetal compromise may contribute to neonatal complications such as:
- Low Apgar scores.
- Respiratory depression.
- Neonatal acidemia.
- Hypoxic-ischemic encephalopathy.
- Seizures in severe cases.
Although uncommon, prolonged oxygen deprivation may ultimately cause serious birth injuries, particularly if intervention is delayed.
Fortunately, modern monitoring practices allow clinicians to identify evolving problems long before permanent injury develops in most cases.
Clinical example
During labor with Pitocin, continuous fetal monitoring demonstrates recurrent late decelerations after the infusion rate is increased. The contraction pattern shows six contractions every 10 minutes with minimal resting time.
The abnormal fetal heart rate tracing reflects reduced placental blood flow caused by excessive uterine activity rather than inadequate labor progression. Immediate reduction of the Pitocin infusion, maternal repositioning, intravenous fluid administration, and supplemental oxygen (when clinically indicated according to institutional protocols) may improve fetal oxygenation while further evaluation is undertaken.
Water Intoxication and Other Serious Adverse Reactions
Although less common than uterine complications, systemic Pitocin side effects can occur because synthetic oxytocin possesses mild antidiuretic activity. This effect resembles that of vasopressin and becomes clinically significant primarily during prolonged infusions involving high doses or excessive administration of electrolyte-free intravenous fluids.
Water intoxication
Water intoxication represents one of the most important systemic complications associated with prolonged Pitocin administration.
The condition develops when excessive free water accumulates within the body, leading to dilutional hyponatremia.
Risk factors include:
- High-dose Pitocin infusion.
- Prolonged administration.
- Large volumes of hypotonic intravenous fluids.
- Delayed recognition of fluid imbalance.
Early symptoms include:
- Headache.
- Nausea.
- Vomiting.
- Fatigue.
- Restlessness.
As hyponatremia worsens, patients may develop:
- Confusion.
- Muscle weakness.
- Visual disturbances.
- Seizures.
- Coma.
Although modern infusion practices have made water intoxication relatively uncommon, healthcare professionals should remain aware of this potentially life-threatening complication.
Uterine rupture
Another rare but devastating Pitocin side effect is uterine rupture.
This complication occurs when excessive uterine force causes disruption of the uterine wall.
Risk factors include:
- Previous uterine surgery.
- Previous cesarean delivery involving a classical incision.
- Obstructed labor.
- Excessive Pitocin dosing.
- Inappropriate Pitocin use despite contraindications.
Clinical features may include:
- Sudden severe abdominal pain.
- Loss of fetal station.
- Abnormal fetal heart rate.
- Maternal hypotension.
- Vaginal bleeding.
- Signs of internal hemorrhage.
Immediate surgical intervention is required because delayed treatment significantly increases maternal and neonatal morbidity.
Postpartum hemorrhage
Although Pitocin is routinely administered after delivery to prevent postpartum hemorrhage, prolonged exposure during labor may occasionally contribute to uterine muscle fatigue.
When the uterus fails to contract effectively after birth (uterine atony), excessive bleeding may occur.
Healthcare providers therefore continue monitoring:
- Uterine tone.
- Vaginal bleeding.
- Maternal vital signs.
- Overall postpartum recovery.
Rare cardiovascular complications
Rare but serious cardiovascular reactions have also been reported, particularly following rapid intravenous administration.
Potential complications include:
- Significant hypotension.
- Cardiac arrhythmias.
- Myocardial ischemia in susceptible patients.
These events reinforce the importance of administering Pitocin intravenously using controlled infusion pumps rather than rapid intravenous boluses during labor.
Importance of Early Recognition
Although severe Pitocin side effects are relatively uncommon in contemporary obstetric practice, they remain clinically significant because deterioration can occur rapidly. Early recognition relies on systematic maternal assessment, continuous evaluation of contraction patterns, vigilant fetal heart rate monitoring, and timely communication among members of the healthcare team.
By understanding both the common and uncommon effects of Pitocin, clinicians are better equipped to recognize subtle changes before they evolve into life-threatening emergencies. Careful dosing, adherence to standardized protocols, and ongoing assessment remain the most effective strategies for minimizing Pitocin side effects and promoting safe outcomes for baby and the mother throughout labor and delivery.
Serious Risks of Pitocin and Birth Injuries
While many Pitocin side effects are mild and resolve with appropriate dose adjustments, some complications have the potential to become obstetric emergencies that threaten the health of both mother and baby. These serious complications are relatively uncommon when Pitocin administration follows evidence-based protocols, but they can occur if the medication is used inappropriately, contraindications are overlooked, or excessive uterine activity is not recognized and corrected promptly.
The primary mechanism behind many severe Pitocin side effects is excessive stimulation of the uterus. Because Pitocin stimulates the myometrium by binding to oxytocin receptors, an excessive response can produce contractions that are too frequent, too prolonged, or too forceful. These abnormal contraction patterns reduce uteroplacental blood flow, impair oxygen delivery to the fetus, increase maternal stress on the uterus, and elevate the risk of maternal and neonatal complications.
Although the term Pitocin and birth injuries is often encountered in legal discussions, it is important to understand that Pitocin itself does not directly cause injury. Rather, birth injuries may occur when excessive uterine activity results in prolonged fetal hypoxia, traumatic delivery, delayed recognition of fetal compromise, or failure to intervene appropriately. Consequently, most serious complications are preventable through careful patient selection, standardized Pitocin induction protocols, continuous maternal and fetal monitoring, and timely clinical intervention.
Several factors increase the likelihood of severe Pitocin side effects, including:
- Excessively rapid dose escalation.
- High dose of Pitocin without adequate reassessment.
- Failure to recognize abnormal uterine contractions.
- Inadequate monitoring of the fetal heart rate.
- Administration despite contraindications.
- Previous uterine surgery.
- Obstructed labor.
- Inappropriate continuation of the Pitocin infusion despite evidence of fetal compromise.
Understanding these risk factors helps healthcare providers identify patients who require closer observation and more cautious management during labor using Pitocin.
Uterine Tachysystole and Hyperstimulation
Among all serious Pitocin side effects, uterine tachysystole is the most frequently encountered complication and often serves as the earliest warning sign of excessive oxytocin activity. If left uncorrected, tachysystole may progress to uterine hyperstimulation, increasing the likelihood of maternal complications and fetal oxygen deprivation.
What is uterine tachysystole?
Uterine tachysystole refers to excessive contraction frequency and is commonly defined as:
- More than five uterine contractions within a 10-minute period, averaged over 30 minutes.
Unlike effective labor, where contractions are separated by adequate resting intervals, tachysystole significantly shortens the time available for uterine relaxation.
Normally, uterine relaxation allows:
- Restoration of placental blood flow.
- Reoxygenation of the fetus.
- Removal of fetal carbon dioxide.
- Recovery of uterine muscle before the next contraction.
When contractions occur too frequently, these restorative processes become progressively compromised.
Understanding uterine hyperstimulation
Although the terms are sometimes used interchangeably, uterine hyperstimulation represents a more severe clinical situation.
Hyperstimulation generally refers to excessive uterine activity that is accompanied by evidence of fetal compromise, such as:
- Persistent uterine contractions with inadequate relaxation.
- Recurrent late decelerations.
- Fetal bradycardia.
- Reduced baseline variability.
- Other abnormal fetal heart rate patterns.
In practical terms, tachysystole describes the contraction pattern, whereas hyperstimulation reflects both excessive contractions and their adverse physiologic impact on the fetus.
Why excessive contractions are dangerous
Each uterine contraction temporarily compresses maternal blood vessels supplying the placenta. Under normal circumstances, blood flow returns between contractions, allowing adequate oxygen exchange.
When Pitocin stimulates contractions too frequently or for prolonged periods:
- Placental perfusion decreases.
- Oxygen delivery to the fetus declines.
- Fetal carbon dioxide accumulates.
- Progressive metabolic acidosis may develop.
- Fetal distress becomes increasingly likely.
If this cycle continues without intervention, prolonged fetal hypoxia may contribute to severe neonatal complications and, in some cases, cause serious birth injuries.
Clinical signs of tachysystole and hyperstimulation
Healthcare providers should immediately evaluate the patient if any of the following occur:
Maternal findings
- Contractions occurring less than two minutes apart.
- Contractions lasting longer than 90 to 120 seconds.
- Minimal uterine relaxation between contractions.
- Severe, persistent abdominal pain.
- Increasing maternal exhaustion.
Fetal findings
- Recurrent late decelerations.
- Persistent fetal bradycardia.
- Reduced fetal heart rate variability.
- Prolonged decelerations.
- Clinical evidence of fetal distress.
Clinical example
A patient undergoing Pitocin induction develops six contractions within a 10-minute period after the infusion rate is increased. Continuous fetal monitoring demonstrates recurrent late decelerations and decreased variability.
These findings indicate uterine tachysystole progressing toward hyperstimulation. The priority is to discontinue or reduce the Pitocin infusion, reposition the patient, improve maternal circulation, and notify the obstetric provider while preparing for additional interventions if fetal compromise persists.
Prompt recognition at this stage often prevents progression to more serious Pitocin side effects.
Uterine Rupture and Postpartum Hemorrhage
Although rare, uterine rupture and postpartum hemorrhage represent two of the most serious maternal complications associated with Pitocin administration. Both conditions require immediate recognition and intervention because delayed treatment may result in severe maternal morbidity or mortality.
Uterine rupture
Uterine rupture is the complete disruption of the uterine wall, allowing communication between the uterine cavity and the abdominal cavity. This complication is considered a true obstetric emergency because it places both the mother and fetus at immediate risk.
While Pitocin alone does not directly cause uterine rupture, excessive uterine stimulation may contribute to rupture in susceptible patients, particularly those with weakened uterine tissue.
Risk factors include:
- Previous classical cesarean incision.
- Prior extensive uterine surgery.
- Previous myomectomy involving the uterine cavity.
- Obstructed labor.
- Excessive uterine stimulation from Pitocin.
- Inappropriate Pitocin use despite contraindications.
Clinical manifestations
Signs and symptoms may include:
- Sudden severe abdominal pain.
- Cessation of previously effective contractions.
- Vaginal bleeding.
- Maternal hypotension.
- Loss of fetal station.
- Abnormal fetal heart rate patterns.
- Signs of internal hemorrhage.
Because fetal compromise often develops before obvious maternal symptoms, continuous fetal monitoring frequently provides the earliest indication of rupture.
Postpartum hemorrhage
Postpartum hemorrhage remains one of the leading causes of maternal morbidity and mortality worldwide. Although Pitocin is given routinely after delivery to prevent uterine atony and reduce bleeding, prolonged exposure during labor may occasionally contribute to uterine muscle fatigue.
An exhausted uterus may fail to contract effectively after delivery, allowing excessive bleeding from the placental implantation site.
Risk factors include:
- Prolonged labor with Pitocin.
- Excessive uterine stimulation.
- Multiple gestation.
- Polyhydramnios.
- Prolonged labor.
- Retained placental tissue.
Clinical signs include:
- Heavy vaginal bleeding.
- Enlarged, soft uterus.
- Tachycardia.
- Hypotension.
- Pallor.
- Decreased urine output.
- Signs of hypovolemic shock in severe cases.
Prompt management includes uterine massage, uterotonic medications, fluid resuscitation, identification of the bleeding source, and escalation of care when necessary.
Importance of prevention
The most effective strategy for preventing both uterine rupture and postpartum hemorrhage is adherence to standardized Pitocin administration protocols. Careful dose titration, recognition of excessive uterine activity, and appropriate patient selection substantially reduce the likelihood of these serious Pitocin side effects.
Pitocin and Birth Injuries: Maternal and Neonatal Complications
The relationship between Pitocin and birth injuries has received considerable attention in both clinical practice and medical-legal settings. However, understanding this relationship requires careful distinction between complications associated with medication use and injuries resulting from inappropriate clinical management.
In most pregnancies, Pitocin contributes to safe labor and delivery without adverse outcomes. Nevertheless, when excessive uterine activity is allowed to continue despite warning signs, the resulting reduction in placental blood flow may increase the risk of maternal and neonatal injury.
Maternal complications
Maternal complications associated with severe Pitocin side effects include:
- Uterine tachysystole.
- Uterine hyperstimulation.
- Uterine rupture.
- Postpartum hemorrhage.
- Emergency cesarean delivery.
- Infection following prolonged labor.
- Increased physical and emotional stress.
- Rarely, hysterectomy following catastrophic hemorrhage.
Many of these complications are secondary to prolonged or excessive uterine activity rather than the medication itself.
Neonatal complications
The fetus depends entirely on maternal circulation for oxygen and nutrient delivery. Therefore, prolonged reductions in placental perfusion can have significant neonatal consequences.
Potential complications include:
- Persistent fetal distress.
- Metabolic acidosis.
- Low Apgar scores.
- Respiratory depression.
- Neonatal seizures.
- Hypoxic-ischemic encephalopathy.
- Multi-organ dysfunction in severe cases.
- Long-term neurodevelopmental impairment in rare situations.
These complications are most often associated with prolonged fetal oxygen deprivation rather than a direct toxic effect of synthetic oxytocin.
Preventing Pitocin-related birth injuries
Preventing Pitocin and birth injuries requires a systematic, evidence-based approach throughout labor induction and labor augmentation.
Key preventive measures include:
- Confirming that Pitocin is clinically indicated before initiation.
- Identifying contraindications before Pitocin administration.
- Using standardized infusion protocols.
- Gradually titrating the dose of Pitocin.
- Continuously assessing contraction patterns.
- Monitoring the fetal heart rate throughout labor.
- Recognizing fetal distress promptly.
- Reducing or discontinuing the Pitocin infusion when excessive uterine activity develops.
- Maintaining effective communication among all members of the obstetric team.
- Documenting assessments, interventions, and patient responses accurately.
Clinical example
A woman undergoing labor induction develops recurrent late decelerations after several increases in the Pitocin infusion. The nurse recognizes the abnormal fetal heart rate pattern, discontinues the infusion according to institutional protocol, repositions the patient, initiates supportive measures, and immediately notifies the obstetric provider. Labor is subsequently completed by emergency cesarean delivery, and the infant is delivered without evidence of hypoxic injury.
This scenario demonstrates that Pitocin side effects do not inevitably result in birth injuries. Rather, prompt recognition, evidence-based nursing interventions, and timely obstetric management are the critical factors that prevent transient complications from progressing to permanent maternal or neonatal harm.
Nursing Assessment and Management During Pitocin Administration
The safe administration of Pitocin extends far beyond initiating an intravenous infusion. Continuous nursing assessment and timely clinical interventions are essential to ensuring that Pitocin achieves its therapeutic goal while minimizing Pitocin side effects. Because the medication directly influences uterine activity, even small changes in the dose of Pitocin may rapidly alter maternal physiology, placental perfusion, and fetal oxygenation. Consequently, nurses serve as the primary clinicians responsible for detecting early changes in maternal and fetal status, implementing evidence-based interventions, and communicating concerns promptly to the obstetric team.
Unlike medications that produce relatively predictable responses, Pitocin requires constant reassessment because the clinical response varies considerably among patients. Some women respond to very low infusion rates, while others require gradual dose escalation before effective labor develops. This variability underscores the importance of individualized care rather than reliance on predetermined dosing schedules.
The overall objectives of nursing management during Pitocin administration include:
- Promoting safe and effective labor induction or labor augmentation.
- Establishing an adequate pattern of uterine contractions without causing excessive uterine activity.
- Maintaining sufficient uteroplacental blood flow.
- Preserving fetal oxygenation.
- Identifying Pitocin side effects before they progress into obstetric emergencies.
- Supporting the physical and emotional well-being of the patient throughout labor and delivery.
- Collaborating effectively with the interdisciplinary healthcare team to optimize maternal and neonatal outcomes.
Achieving these objectives requires systematic maternal and fetal assessment throughout every phase of the Pitocin infusion, from initiation until delivery.
Maternal and Fetal Monitoring
Continuous monitoring is the cornerstone of safe Pitocin administration. Because the medication has a rapid onset of action when administered intravenously, maternal and fetal conditions can change within minutes following dose adjustments. Ongoing assessment enables healthcare providers to identify subtle physiologic changes before they develop into severe Pitocin side effects.
Maternal assessment before initiating Pitocin
Before beginning Pitocin infusion, nurses should perform a comprehensive baseline assessment to determine whether the patient is an appropriate candidate for therapy and to establish reference values for subsequent comparisons.
The initial assessment should include:
Maternal history
Important aspects include:
- Previous pregnancies and deliveries.
- Previous cesarean section or uterine surgery.
- History of uterine rupture.
- Obstetric complications.
- Medical disorders such as hypertension or diabetes.
- Allergies and medication history.
- Indication for Pitocin induction.
This information helps identify factors that may increase the risks associated with Pitocin.
Physical assessment
Baseline evaluation includes:
- Blood pressure.
- Heart rate.
- Respiratory rate.
- Temperature.
- Pain assessment.
- Hydration status.
- Presence of vaginal bleeding.
- Uterine activity.
- Cervical examination findings.
- Membrane status.
These findings provide important reference points throughout labor.
Baseline fetal assessment
Prior to initiating Pitocin, fetal evaluation should confirm that the fetus is tolerating labor appropriately.
Assessment includes:
- Baseline fetal heart rate.
- Heart rate variability.
- Accelerations.
- Presence or absence of decelerations.
- Fetal presentation and station.
Abnormal baseline findings may require further evaluation before Pitocin administration proceeds.
Ongoing maternal monitoring during labor
Once Pitocin is administered, maternal assessment becomes a continuous process rather than a single event.
Nurses should regularly evaluate:
Vital signs
Routine monitoring includes:
- Blood pressure.
- Heart rate.
- Respiratory status.
- Oxygen saturation when clinically indicated.
- Temperature during prolonged labor.
Changes in maternal vital signs may indicate complications such as infection, hypotension, or hemorrhage.
Uterine activity
Continuous evaluation of uterine activity is essential because excessive stimulation represents one of the most important Pitocin side effects.
Assessment should include:
- Frequency of contractions.
- Duration of each contraction.
- Intensity.
- Resting uterine tone.
- Presence of adequate relaxation between contractions.
Effective labor generally consists of contractions that occur regularly while allowing sufficient recovery time for restoration of placental blood flow.
Fluid balance
Although uncommon, prolonged Pitocin infusion may contribute to water intoxication because oxytocin is a hormone with mild antidiuretic properties.
Nurses should monitor:
- Intravenous fluid intake.
- Urine output.
- Signs of fluid overload.
- Neurologic status when prolonged infusions are required.
Early identification of fluid imbalance reduces the likelihood of severe systemic Pitocin side effects.
Continuous fetal monitoring
Because the fetus depends entirely on placental circulation for oxygen delivery, continuous fetal assessment is equally important during Pitocin administration.
Electronic fetal monitoring allows clinicians to evaluate the fetal response to labor in real time.
Important parameters include:
Baseline fetal heart rate
Normal baseline values provide an important indicator of fetal well-being before and throughout labor.
Heart rate variability
Moderate variability generally reflects adequate fetal oxygenation and intact neurologic function.
Reduced variability may indicate:
- Fetal hypoxia.
- Medication effects.
- Sleep cycles.
- Progressive compromise when accompanied by other abnormalities.
Accelerations
Accelerations are generally reassuring and suggest an appropriately oxygenated fetus.
Decelerations
Nurses should distinguish between:
- Early decelerations.
- Variable decelerations.
- Late decelerations.
- Prolonged decelerations.
Late decelerations are particularly concerning because they frequently indicate uteroplacental insufficiency resulting from reduced placental blood flow.
Example of effective monitoring
A woman receiving Pitocin to induce labor demonstrates:
- Four contractions every 10 minutes.
- Moderate contraction intensity.
- Normal uterine relaxation between contractions.
- Baseline fetal heart rate of 140 beats per minute.
- Moderate variability.
- Occasional accelerations.
These findings indicate that the Pitocin infusion is producing effective labor while maintaining reassuring maternal and fetal status.
Recognizing Abnormal Contraction Patterns and Fetal Distress
One of the most important nursing responsibilities during Pitocin administration is recognizing when normal labor transitions into excessive uterine activity or fetal compromise. Early identification allows prompt intervention before temporary physiologic changes progress into severe Pitocin side effects or Pitocin and birth injuries.
Abnormal contraction patterns
Contractions should facilitate cervical dilation without excessively reducing uteroplacental perfusion.
Warning signs include:
Uterine tachysystole
Defined as:
- More than five uterine contractions within 10 minutes.
Prolonged contractions
Contractions lasting longer than 90–120 seconds may significantly reduce placental blood flow.
Elevated resting uterine tone
Failure of the uterus to relax adequately between contractions limits fetal oxygenation and increases maternal discomfort.
Hyperstimulation
Hyperstimulation occurs when excessive uterine activity is accompanied by evidence of fetal compromise.
This represents one of the most serious Pitocin side effects because continued oxygen deprivation increases the likelihood of neonatal injury.
Recognizing fetal distress
Fetal distress develops when the fetus no longer tolerates labor adequately.
Clinical indicators include:
- Persistent late decelerations.
- Fetal bradycardia.
- Minimal or absent variability.
- Recurrent prolonged decelerations.
- Sinusoidal fetal heart rate pattern (rare but serious).
These findings require immediate evaluation of the Pitocin infusion and maternal condition.
Clinical example
A patient undergoing labor using Pitocin initially progresses normally. After the infusion rate is increased, contractions begin occurring every 90 seconds, lasting approximately two minutes each. Continuous monitoring demonstrates recurrent late decelerations and minimal fetal heart rate variability.
These findings indicate excessive uterine activity with evolving fetal distress. Without prompt intervention, prolonged fetal hypoxia may increase the risk of severe neonatal complications.
Nursing Interventions for Pitocin Side Effects
Recognizing Pitocin side effects is only the first step; prompt nursing intervention is essential to prevent progression to maternal or fetal emergencies. Evidence-based interventions focus on restoring adequate uteroplacental perfusion, improving fetal oxygenation, correcting excessive uterine activity, and facilitating rapid interdisciplinary communication.
Immediate interventions for excessive uterine activity
When tachysystole or hyperstimulation develops, nurses should act immediately according to institutional protocols.
Common interventions include:
1. Reduce or discontinue the Pitocin infusion
Because excessive uterine activity is often dose-related, decreasing or stopping the Pitocin infusion is usually the first intervention.
This reduces stimulation of oxytocin receptors and allows the uterus to relax.
2. Reposition the patient
Positioning the patient in the left lateral position helps improve maternal circulation and enhances placental blood flow.
3. Increase intravenous fluids when indicated
Appropriate fluid administration may improve maternal blood volume and uteroplacental perfusion, provided fluid overload is not present.
4. Notify the obstetric provider immediately
Persistent abnormal findings require rapid interdisciplinary communication to determine whether additional interventions or operative delivery are necessary.
Interventions for fetal distress
When evidence of fetal distress develops, nursing priorities include restoring fetal oxygenation while preparing for possible escalation of care.
Management may include:
- Continuous evaluation of the fetal heart rate.
- Discontinuation of Pitocin administration.
- Maternal repositioning.
- Intravenous fluid administration when appropriate.
- Preparation for emergency delivery if fetal compromise persists despite corrective measures.
Institutional policies and current clinical guidelines should always guide the use of supplemental oxygen and other supportive therapies.
Ongoing maternal assessment
Following any intervention, nurses should reassess:
- Contraction frequency.
- Contraction duration.
- Maternal vital signs.
- Pain level.
- Vaginal bleeding.
- Uterine relaxation.
- Overall labor progress.
These reassessments determine whether interventions have successfully reduced Pitocin side effects.
Documentation
Accurate documentation is a critical component of nursing management.
Documentation should include:
- Indication for Pitocin use.
- Initial and subsequent dose of Pitocin.
- Time of dose adjustments.
- Maternal assessment findings.
- Fetal heart rate interpretations.
- Contraction characteristics.
- Nursing interventions performed.
- Patient responses.
- Communication with healthcare providers.
Comprehensive documentation supports continuity of care, facilitates interdisciplinary communication, promotes quality improvement, and provides an accurate legal record of clinical decision-making.
Patient education and emotional support
Nursing management extends beyond physiologic assessment. Women receiving Pitocin often experience anxiety related to labor induction, stronger contractions, or unexpected changes in the birth plan.
Nurses should:
- Explain the purpose of Pitocin administration.
- Describe expected labor progression.
- Discuss potential Pitocin side effects in understandable language.
- Encourage questions and shared decision-making whenever appropriate.
- Provide reassurance while maintaining honest communication regarding labor progress and clinical findings.
Clear communication helps reduce anxiety, improves patient cooperation, and strengthens trust between the healthcare team and the patient.
Ultimately, effective nursing assessment and management during Pitocin administration combine vigilant monitoring, timely recognition of abnormal findings, evidence-based clinical interventions, accurate documentation, and compassionate patient-centered care. These responsibilities are fundamental to reducing Pitocin side effects, preventing serious maternal and neonatal complications, and promoting safe, high-quality outcomes throughout labor and delivery.
Safe Pitocin Use, Guidelines, and Legal Considerations
The widespread use of Pitocin has transformed modern obstetric care by providing clinicians with an effective method to induce labor, augment labor, and reduce the risk of postpartum hemorrhage. However, because Pitocin directly influences uterine activity and fetal oxygenation, it is also recognized as a medication that requires meticulous administration and continuous monitoring. While Pitocin side effects are often preventable, inappropriate dosing, failure to recognize excessive uterine activity, inadequate fetal monitoring, or delayed clinical intervention can result in serious maternal and neonatal complications.
For this reason, healthcare organizations have established comprehensive safety recommendations that govern every aspect of Pitocin administration, from patient selection and infusion protocols to documentation and interdisciplinary communication. These recommendations are supported by regulatory agencies, professional organizations, and patient safety experts whose primary objective is to improve the safety of both the mother and fetus throughout labor and delivery.
Safe Pitocin use is based on several fundamental principles:
- Administer Pitocin only when there is a clear medical indication.
- Carefully evaluate maternal and fetal contraindications before initiating therapy.
- Use standardized Pitocin induction protocols.
- Begin with the lowest effective dose of Pitocin.
- Increase the infusion gradually based on clinical response.
- Continuously monitor maternal status, uterine contractions, and fetal heart rate.
- Recognize Pitocin side effects promptly.
- Document assessments and interventions accurately.
- Communicate abnormal findings immediately to the obstetric provider.
- Discontinue or reduce the Pitocin infusion when excessive uterine activity or fetal distress develops.
Adhering to these principles substantially reduces the risks associated with Pitocin while maximizing its therapeutic benefits.
Food and Drug Administration Warnings for Pitocin
The Food and Drug Administration (FDA) has approved Pitocin for specific obstetric indications, including labor induction, labor augmentation, and management of postpartum uterine atony. However, the agency also recognizes that inappropriate Pitocin use can produce significant maternal and fetal complications. Consequently, the FDA-approved prescribing information contains several important precautions and warning for Pitocin that healthcare professionals must understand before administering the medication.
FDA-approved indications
According to the Food and Drug Administration, Pitocin is used in carefully selected patients for purposes such as:
- Induce labor when continuation of pregnancy presents greater risk than delivery.
- Augment inadequate labor.
- Improve ineffective uterine contractions.
- Reduce bleeding following delivery by promoting uterine contraction.
These indications emphasize that Pitocin should be administered only when there is an appropriate clinical justification rather than for convenience or elective scheduling without medical necessity.
Major FDA warnings
The FDA highlights several important safety concerns regarding Pitocin administration.
Excessive uterine activity
One of the most significant Pitocin side effects is excessive stimulation of the uterus, which may result in:
- Uterine tachysystole.
- Hyperstimulation.
- Reduced placental blood flow.
- Fetal distress.
- Uterine rupture in susceptible patients.
These complications underscore the importance of gradual dose titration and continuous assessment throughout the Pitocin infusion.
Continuous fetal monitoring
The FDA recommends careful observation of both maternal and fetal status during labor using Pitocin.
Continuous assessment should include:
- Frequency of uterine contractions.
- Duration of contractions.
- Resting uterine tone.
- Maternal vital signs.
- Continuous fetal heart rate monitoring whenever appropriate.
Abnormal findings should prompt immediate reassessment of the infusion and implementation of corrective measures.
Contraindications
The FDA also specifies situations in which Pitocin should not be administered.
Examples include:
- Placenta previa.
- Umbilical cord prolapse.
- Abnormal fetal presentation incompatible with vaginal delivery.
- Previous classical cesarean incision.
- Situations in which vaginal birth is contraindicated.
Administering Pitocin despite these contraindications substantially increases the risk of serious maternal complications.
Institute for Safe Medication Practices recommendations
The Institute for Safe Medication Practices (ISMP) classifies Pitocin as a high-alert medication because dosing errors or inappropriate administration can have immediate and potentially catastrophic consequences.
ISMP recommendations include:
- Standardized infusion concentrations.
- Electronic infusion pumps.
- Independent double verification before initiation.
- Standardized dose adjustment protocols.
- Ongoing competency training for healthcare providers.
- Immediate access to emergency obstetric interventions.
These recommendations are designed to reduce medication errors and improve patient safety throughout Pitocin administration.
Professional guideline recommendations
Professional organizations such as the American College of Obstetricians and Gynecologists (ACOG) and the Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) also emphasize evidence-based approaches to Pitocin use.
Common recommendations include:
- Individualized patient assessment before induction.
- Continuous evaluation of maternal and fetal responses.
- Avoidance of unnecessary dose escalation.
- Prompt recognition of Pitocin side effects.
- Standardized communication among healthcare team members.
- Regular review of institutional induction protocols.
Together, these recommendations support consistent, evidence-based obstetric practice.
Documentation and Best Practices for Safe Pitocin Administration
Accurate documentation is one of the most important professional responsibilities associated with Pitocin administration. Comprehensive documentation supports patient safety, facilitates communication among healthcare providers, promotes continuity of care, and provides an accurate record of clinical decision-making.
In addition, documentation serves an essential quality improvement and legal function by demonstrating adherence to accepted standards of care.
Essential documentation before Pitocin initiation
Prior to beginning the Pitocin infusion, documentation should include:
- Medical indication for labor induction or augmentation.
- Maternal informed consent according to institutional policy.
- Baseline maternal assessment.
- Baseline fetal heart rate assessment.
- Cervical examination findings.
- Membrane status.
- Confirmation that contraindications have been excluded.
- Initial dose of Pitocin prescribed.
These baseline findings establish the patient’s condition before medication administration.
Documentation during Pitocin administration
Throughout the infusion, documentation should be continuous and objective.
Important information includes:
Medication administration
Record:
- Infusion start time.
- Infusion rate.
- Every dose adjustment.
- Time of each adjustment.
- Reason for increasing or decreasing the infusion.
- Time of discontinuation when applicable.
Maternal assessment
Document:
- Blood pressure.
- Heart rate.
- Respiratory rate.
- Pain assessment.
- Uterine activity.
- Labor progression.
- Presence of Pitocin side effects.
Fetal assessment
Documentation should include:
- Baseline fetal heart rate.
- Variability.
- Accelerations.
- Decelerations.
- Overall interpretation of fetal status.
Objective fetal assessment provides valuable evidence supporting clinical decision-making throughout labor.
Nursing interventions
Whenever abnormal findings occur, nurses should document:
- Assessment findings.
- Nursing interventions performed.
- Provider notification.
- Orders received.
- Patient response.
- Subsequent reassessment.
This chronological documentation demonstrates timely recognition and management of developing complications.
Best practices for safe Pitocin administration
Safe Pitocin administration extends beyond documentation alone.
Evidence-based best practices include:
Patient selection
Only use Pitocin to induce labor when clear maternal or fetal indications exist.
Careful patient selection reduces unnecessary exposure to Pitocin side effects.
Standardized protocols
Healthcare organizations should utilize standardized Pitocin induction protocols that specify:
- Initial dosing.
- Dose escalation intervals.
- Maximum infusion rates.
- Criteria for discontinuation.
- Required monitoring parameters.
Standardization minimizes practice variation and reduces medication errors.
Interdisciplinary communication
Effective communication among nurses, obstetricians, midwives, anesthesiologists, and neonatal providers is essential throughout labor and delivery.
Early communication regarding:
- Abnormal contraction patterns.
- Fetal distress.
- Failure of labor progression.
- Maternal deterioration.
allows prompt intervention before complications worsen.
Ongoing education
Healthcare professionals should participate in regular continuing education addressing:
- Pitocin side effects.
- Interpretation of fetal heart rate tracings.
- Emergency obstetric management.
- Medication safety.
- Updated clinical guidelines.
Continual education helps maintain clinical competence and improves patient outcomes.
Pitocin, Birth Injuries, and the Role of a Birth Injury Attorney
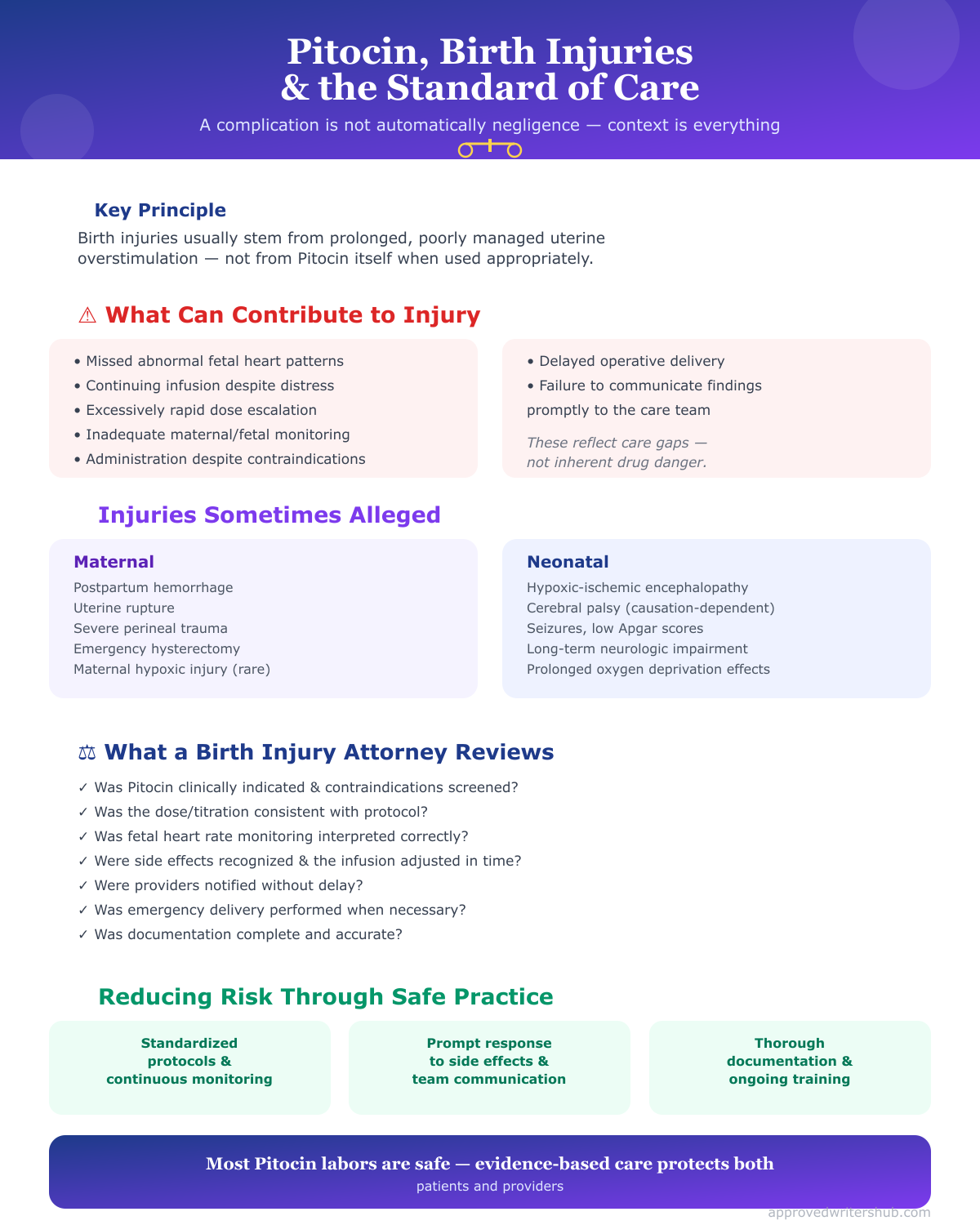
Discussions regarding Pitocin and birth injuries frequently arise when adverse maternal or neonatal outcomes occur during labor and delivery. It is important to recognize, however, that the occurrence of a complication does not automatically indicate negligence or inappropriate care. Obstetric practice involves managing complex clinical situations in which complications may develop despite appropriate assessment, timely interventions, and adherence to accepted standards of care.
From a clinical perspective, Pitocin and birth injuries are most often associated with prolonged or inadequately managed excessive uterine activity rather than the medication itself. When Pitocin side effects such as uterine tachysystole or hyperstimulation are recognized early and managed promptly, most patients experience favorable outcomes without permanent maternal or neonatal injury.
Circumstances that may contribute to birth injuries
Examples of situations that may increase the risk of birth injuries include:
- Failure to recognize abnormal fetal heart rate patterns.
- Continuing Pitocin infusion despite persistent fetal distress.
- Excessively rapid dose escalation.
- Inadequate monitoring of maternal or fetal status.
- Administration despite contraindications.
- Delayed operative delivery when clinically indicated.
- Failure to communicate critical findings promptly.
These situations emphasize the importance of evidence-based clinical practice rather than suggesting that Pitocin itself is inherently unsafe.
Common injuries discussed in cases involving Pitocin
In some cases involving Pitocin, alleged injuries may involve:
Maternal complications
- Postpartum hemorrhage.
- Uterine rupture.
- Severe perineal trauma.
- Emergency hysterectomy.
- Maternal hypoxic injury in rare circumstances.
Neonatal complications
- Hypoxic-ischemic encephalopathy.
- Cerebral palsy resulting from prolonged hypoxia (where causation is established).
- Seizures.
- Low Apgar scores.
- Long-term neurologic impairment.
- Other birth injuries related to prolonged oxygen deprivation.
Importantly, these outcomes have multiple potential causes. Determining whether Pitocin administration contributed requires careful review of the complete clinical record, fetal monitoring data, maternal history, timing of events, and adherence to accepted standards of care.
The role of a birth injury attorney
When families believe that preventable medical errors contributed to maternal or neonatal harm, they may consult a birth injury attorney. Attorneys who handle obstetric malpractice cases typically evaluate whether the healthcare team met the applicable standard of care during pregnancy, labor induction, Pitocin administration, and delivery.
A legal review often focuses on questions such as:
- Was Pitocin clinically indicated?
- Were contraindications identified appropriately?
- Was the dose of Pitocin consistent with accepted protocols?
- Were maternal assessments performed appropriately?
- Was continuous fetal heart rate monitoring interpreted correctly?
- Were Pitocin side effects recognized promptly?
- Was the Pitocin infusion reduced or discontinued when indicated?
- Were obstetric providers notified without unnecessary delay?
- Was emergency delivery performed when clinically necessary?
- Was documentation complete and accurate?
These questions are evaluated using medical records, fetal monitoring strips, institutional policies, expert testimony, and evidence-based clinical guidelines.
Reducing legal risk through safe clinical practice
The most effective way to reduce both patient harm and legal exposure is consistent adherence to evidence-based standards of care. Healthcare professionals should focus on preventing complications through vigilant assessment, timely intervention, and accurate documentation rather than practicing defensively.
Key risk-reduction strategies include:
- Following standardized Pitocin administration protocols.
- Maintaining continuous maternal and fetal monitoring.
- Recognizing and responding promptly to Pitocin side effects.
- Communicating concerns immediately to the interdisciplinary team.
- Documenting assessments, interventions, and patient responses objectively and thoroughly.
- Participating in ongoing education and simulation training related to obstetric emergencies.
Ultimately, the overwhelming majority of women who receive Pitocin experience safe labor and delivery when evidence-based practices are followed. Understanding current safety recommendations, regulatory guidance, meticulous documentation standards, and the legal implications of obstetric care equips healthcare professionals to provide high-quality, patient-centered care while minimizing the risks associated with Pitocin and reducing the likelihood of preventable maternal or neonatal birth injuries.
Conclusion
Pitocin has become one of the most important medications in modern obstetric practice, playing a vital role in labor induction, labor augmentation, and the prevention of postpartum hemorrhage. As a synthetic form of oxytocin, it has significantly improved maternal and neonatal outcomes by helping initiate or strengthen uterine contractions when spontaneous labor is absent or ineffective. However, like any high-alert medication, its benefits are closely tied to appropriate clinical use. Understanding Pitocin side effects is essential because the same medication that facilitates a safe vaginal birth can also contribute to serious maternal and fetal complications if administered without careful assessment, standardized protocols, and continuous monitoring.
Throughout this guide, it has become evident that the safe administration of Pitocin requires far more than simply initiating an intravenous infusion. Effective Pitocin use begins with selecting appropriate candidates for labor induction, recognizing contraindications, and understanding the pharmacologic effects of oxytocin on the uterus. Equally important is appreciating how Pitocin stimulates uterine activity, influences placental blood flow, and affects fetal oxygenation. This knowledge provides the foundation for recognizing both the expected therapeutic effects and the early signs of Pitocin side effects, enabling healthcare professionals to intervene before complications escalate.
A recurring theme throughout obstetric care is the importance of balancing effective labor progression with maternal and fetal safety. Excessive uterine activity, including tachysystole and hyperstimulation, can compromise placental perfusion and increase the likelihood of fetal distress, uterine rupture, postpartum hemorrhage, and, in severe cases, Pitocin and birth injuries. Fortunately, these complications are often preventable through evidence-based practices such as gradual dose titration, continuous assessment of uterine contractions, vigilant fetal heart rate monitoring, timely nursing interventions, and effective interdisciplinary communication.
Nurses occupy a central position in maintaining the safety of mother and baby during labor and delivery. Their responsibilities extend beyond medication administration to include comprehensive maternal and fetal assessment, recognition of abnormal contraction patterns, interpretation of fetal monitoring data, implementation of appropriate interventions, patient education, and meticulous documentation. By integrating clinical judgment with current evidence-based guidelines, nurses play an indispensable role in reducing Pitocin side effects, preventing avoidable complications, and promoting positive birth outcomes.
Safe Pitocin administration also depends on adherence to recommendations established by organizations such as the Food and Drug Administration, the Institute for Safe Medication Practices, and professional obstetric associations. These evidence-based guidelines emphasize standardized induction protocols, careful patient selection, accurate documentation, and continuous quality improvement to minimize the risks associated with Pitocin. Healthcare providers who consistently apply these principles strengthen patient safety while fostering a culture of accountability and excellence in obstetric care.
Ultimately, Pitocin remains an invaluable medication when used appropriately and responsibly. Its success lies not only in its ability to stimulate uterine contractions but also in the knowledge, vigilance, and clinical expertise of the healthcare professionals who administer it. By developing a thorough understanding of Pitocin side effects, recognizing early warning signs of maternal and fetal compromise, and applying evidence-based nursing management strategies, clinicians can maximize the therapeutic benefits of Pitocin while minimizing potential harm. This commitment to safe practice helps ensure that every woman receives high-quality, patient-centered care and that every newborn is given the safest possible start in life.
Frequently Asked Questions
What are the risks of getting Pitocin?
Pitocin is generally safe when used appropriately, but it can cause side effects and complications, particularly if uterine contractions become too frequent or too strong. Potential risks include:
- Uterine tachysystole (excessively frequent contractions)
- Fetal distress due to reduced placental blood flow
- Changes in the fetal heart rate
- Uterine rupture (rare, especially in women with previous uterine surgery)
- Postpartum hemorrhage
- Water intoxication and hyponatremia with prolonged high-dose infusions (rare)
Continuous maternal and fetal monitoring helps detect these complications early and allows prompt intervention.
Why would you refuse Pitocin?
A patient may choose to decline Pitocin after discussing the benefits, risks, and alternatives with their healthcare provider. Common reasons include:
- Preference for spontaneous labor without medical intervention
- Desire for a low-intervention or unmedicated birth
- Concerns about stronger or more frequent contractions
- Previous negative experience with labor induction
- Medical situations where Pitocin is contraindicated or another management approach is more appropriate
The decision should always be made through informed, shared decision-making between the patient and the healthcare team.
What to expect when induced with Pitocin?
When labor is induced with Pitocin, the medication is administered intravenously using an infusion pump. During the process, you can expect:
- A low starting dose that is gradually increased until an effective contraction pattern develops
- Continuous monitoring of contractions and the baby’s heart rate
- Regular assessment of cervical dilation and labor progress
- Dose adjustments based on how both the mother and baby respond
- The possibility of additional interventions, such as artificial rupture of membranes, if clinically indicated
The duration of induction varies widely and depends on cervical readiness, individual response to Pitocin, and whether it is being used to induce or augment labor.
Are inductions more painful?
They can be. Pitocin-induced contractions are often stronger, more regular, and closer together than contractions during spontaneous labor, which may make labor feel more intense. However, pain experiences vary greatly from person to person.
Many women successfully manage induced labor using breathing techniques, movement, hydrotherapy, or other comfort measures, while others choose pain relief options such as epidural anesthesia. Regardless of the method, healthcare providers continuously monitor both the mother and baby to promote a safe labor and delivery.