Episodic/Focused SOAP Note for Patient with Allergic Rhinitis
Episodic/Focused SOAP Note for Patient with Allergic Rhinitis
(Episodic/Focused SOAP Note for Patient with Allergic Rhinitis)
Patient Information:
S.
CC: “I get this every spring and it seems to last six to eight weeks”
HPI: The patient is a 28-year-old Hispanic female presenting at the clinic complaining of a runny nose and itchy eyes. The patient states runny nose, itchy eyes, and ears felt full approximately 9 days ago. The patient reports experiencing this condition every spring, which lasts six to eight weeks”. She describes the nose as runny with clear mucus. Sneezes on and off all day. Her eyes itch so bad she just wants to scratch them out, sometimes feels a tickle in her throat, and her ears feel full and sometimes pop. Last year she took Claritin with relief.
Current Medications: Acetaminophen 325mg
Allergies: Dust and pollen.
PMHx: Positive history of Covid-19, controlled and vaccinated.
FH: Father at 66 has a history of kidney stones. Mother died when 37 from accident, and not known medical history
Soc Hx: Negative history of tobacco, alcohol, or substance use. Married and living with the husband.
ROS
GENERAL: Denies weight loss, fever, chills, weakness or fatigue.
HEENT: Eyes: Denies visual loss, blurred vision, double vision or yellow sclerae. Reports itchy eyes.
Ears, Nose, Throat: Denies hearing loss. Reports feelings ears are full. Reports sneezing and denies congestion. Reports runny nose and scratchy throat. Throat mildly erythematous.
SKIN: Denies rash or itching.
CARDIOVASCULAR: Denies chest pain, chest pressure or chest discomfort. No palpitations or edema.
RESPIRATORY: Reports shortness of breath due to blocked airways, sneezing on and off throughout the day. Denies cough or sputum.
GASTROINTESTINAL: Denies anorexia, nausea, vomiting or diarrhea. No abdominal pain or blood.
GENITOURINARY: Denies burning on urination, pregnancy. Last menstrual period, 27/02/2023.
NEUROLOGICAL: Denies headache, dizziness, syncope, paralysis, ataxia, numbness or tingling in the extremities. No change in bowel or bladder control.
MUSCULOSKELETAL: Denies muscle, back pain, joint pain or stiffness.
HEMATOLOGIC: Denies anemia, bleeding or bruising.
LYMPHATICS: Denies enlarged nodes. No history of splenectomy.
PSYCHIATRIC: Denies history of depression or anxiety.
ENDOCRINOLOGIC: Denies reports of sweating, cold or heat intolerance. No polyuria or polydipsia.
ALLERGIES: Dust and pollen.
O.
VS: Temp: 97.8F, B.P.: 110/70, P: 85, R.R.: 19, O2: Room air, Pain: 0/10, Ht: 5’9 feet, Wt: 170 lbs, BMI: 25.1, BMI Range: Overweight
Physical exam: Alert and oriented
HEENT: Her throat was mildly erythematous without exudate. Nasal mucosa was pale, boggy, and erythematous, with clear thin secretions and enlarged nasal turbinates. Only clear drainage was seen. TMs were clear.
Neck: Supple without adenopathy.
Lungs: Clear.
A.
Differential Diagnoses:
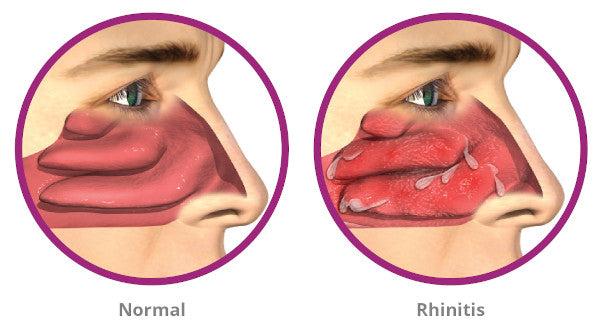
1) Allergic Rhinitis: Allergic rhinitis occurs in the eyes, nose, and throat when airborne allergens cause the body to release histamine. Pollen, dust mites, mold, cockroach feces, animal dander, fumes and aromas, hormonal fluctuations, and smoke are some of the most typical triggers of rhinitis. Sneezing, a stuffy, runny, and itchy nose, itchy throat, eyes, and ears, nosebleeds, clear drainage from the nose, recurrent ear infections, snoring, mouth breathing, and fatigue are all signs of allergic rhinitis (Akhouri et al., 2022). The patient presents with itchy eyes and ears, a runny nose with clear discharge, and a sore or itchy throat, guiding the diagnosis of allergic rhinitis, which seems to affect the patient only in spring, implying pollen-induced allergic rhinitis.
2) Vasomotor rhinitis: The most prevalent type of nonallergic rhinitis, vasomotor rhinitis, is diagnosed as an exclusion. Nonallergic rhinitis has a complicated pathogenesis that is still being studied (Leader & Geiger, 2022). The nasal mucosa’s parasympathetic and sympathetic inputs are out of balance, contributing to this condition. In allergic and nonallergic rhinitis, headache, face pressure, postnasal drip, coughing, and throat clearing are typical symptoms. According to the predominating symptomatology, patients with vasomotor rhinitis are typically divided into “blocks” with congestion and “runners” with rhinorrhea. Rhinorrhea patients frequently exhibit an intensified cholinergic response (Leader & Geiger, 2022). Nociceptive neurons in people with nasal blockage may respond more strongly to benign stimuli. This diagnosis was refuted because the patient clearly indicated she experiences the symptoms during spring; hence the cause is known.
(Episodic/Focused SOAP Note for Patient with Allergic Rhinitis)
3) Acute Sinusitis: Acute sinusitis is an infection of the sinuses. It involves sinus passageways and nasal passages, which are connected. Purulent nasal discharge, along with either a nasal blockage or discomfort, pressure, or fullness in the face, are the three core symptoms that are the most sensitive and specific for acute rhinosinusitis (DeBoer & Kwon, 2019). Patients who could present with general “headache” concerns help to clarify this because an isolated headache is not a symptom. However, sinusitis can be characterized by isolated facial pressure. This diagnosis was refuted because the nasal discharge was clear.
4) Rhinitis Medicamentosa: Rebound congestion, commonly called “rebound rhinitis medicamentosa,” is an inflammation of the nasal mucosa brought on by excessive consumption of topical nasal decongestants. It is categorized as a form of drug-induced rhinitis. While using an intranasal decongestant for an extended period of time, the patient often experiences a recurrence of nasal congestion, especially without rhinorrhea (Wahid & Shermetaro, 2021). Snoring, oral breathing, and dry mouth are all symptoms of severe nasal congestion. A clinical examination will show swollen, erythematous, and granular nasal mucosa. Furthermore, pale and edematous looks can be noticed (Wahid & Shermetaro, 2021). The nasal membrane is crusty and atrophic as the condition worsens. The diagnosis was refuted because the cause is established as pollen common during spring and not any medication.
(Episodic/Focused SOAP Note for Patient with Allergic Rhinitis)
5) Hormone-Induced Rhinitis: Hormone-induced rhinitis is marked by congestion and nasal symptoms brought on by endogenous female hormones, such as those present during pregnancy. Patients with a history of craniofacial trauma or prior facial surgery with persistent, clear rhinorrhea should be evaluated for a cerebrospinal fluid (CSF) leak (Liva et al., 2021). This diagnosis was ruled out because the patient denied pregnancy, minimizing the likelihood of being affected by endogenous female hormones. Also, the patient has no surgical history.
This section is not required for the assignments in this course (NURS 6512) but will be required for future courses.
References
Akhouri, S., House, S. A., & Doerr, C. (2022). Allergic rhinitis (nursing). In StatPearls [Internet]. StatPearls Publishing.
DeBoer, D. L., & Kwon, E. (2019). Acute sinusitis. In StatPearls [Internet]. StatPearls Publishing.
Leader, P., & Geiger, Z. (2022). Vasomotor rhinitis. In StatPearls [Internet]. StatPearls Publishing.
Liva, G. A., Karatzanis, A. D., & Prokopakis, E. P. (2021). Review of Rhinitis: Classification, Types, Pathophysiology. Journal of clinical medicine, 10(14), 3183. https://doi.org/10.3390/jcm10143183
Wahid, N. W. B., & Shermetaro, C. (2021). Rhinitis medicamentosa. In StatPearls [Internet]. StatPearls Publishing.

