Comprehensive Nursing Paper on Allergies: Understanding, Management, and Education
Comprehensive Nursing Paper on Allergies: Understanding, Management, and Education
 Causes
Causes
Allergies arise from a combination of genetic predispositions and environmental factors. Genetic susceptibility plays a significant role, with individuals inheriting a predisposition to develop allergies from their parents. Specific genetic variations influence immune system responses, making certain individuals more prone to allergic reactions.
Environmental factors also contribute significantly to the development of allergies. Exposure to allergens in the environment, such as pollen, dust mites, mold, pet dander, and certain foods, can trigger immune system responses in susceptible individuals. These allergens are substances that are typically harmless to most people but provoke an abnormal reaction in those with allergies.
:max_bytes(150000):strip_icc()/VWH_Illustration_Allergen-Types-and-Triggers_Illustrator_Sydney-Saporito_Final-00bb7f7393d6436e9dc347e85a0ec0b3.jpg)
Furthermore, early childhood exposure to allergens may influence the development of allergies later in life. Studies suggest that early exposure to certain allergens, particularly in infancy and early childhood, may either increase or decrease the likelihood of developing allergies. This phenomenon is known as the “hygiene hypothesis,” which suggests that reduced exposure to infectious agents and microbial organisms in early childhood may lead to an increased risk of developing allergies.
Additionally, environmental factors such as pollution and climate change can exacerbate allergic reactions. Airborne pollutants, including vehicle emissions and industrial pollutants, can worsen allergy symptoms by irritating the respiratory system and enhancing the effects of allergens. Climate change can also impact the distribution and concentration of allergens, prolonging allergy seasons and increasing exposure levels.
In summary, allergies have multifaceted causes involving a combination of genetic predispositions and environmental influences. Understanding these factors is crucial for identifying triggers, implementing preventive measures, and developing effective treatment strategies for allergy management. (Comprehensive Nursing Paper on Allergies: Understanding, Management, and Education)
Signs and Symptoms
Allergic reactions manifest through a diverse range of signs and symptoms, varying in severity from mild discomfort to life-threatening reactions. The presentation of symptoms depends on the type of allergen, the route of exposure, and individual factors such as genetic predispositions and immune system sensitivity.
Common signs and symptoms of allergic reactions include:
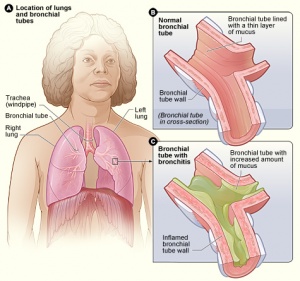
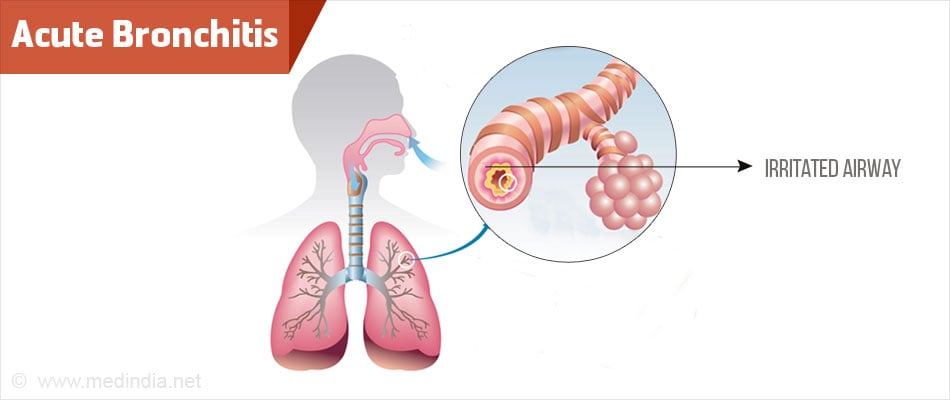
- Respiratory Symptoms: Allergies often affect the respiratory system, leading to symptoms such as sneezing, nasal congestion, runny nose, coughing, and wheezing. These symptoms are typical of allergic rhinitis or hay fever, which is triggered by allergens like pollen, dust mites, or pet dander.
- Skin Reactions: Allergic reactions can cause various skin manifestations, including itching, redness, hives (urticaria), and eczema (atopic dermatitis). These symptoms typically occur after direct contact with allergens or through systemic exposure, such as ingestion or inhalation.

- Ocular Symptoms: Allergies commonly affect the eyes, leading to symptoms such as redness, itching, watering (tearing), and swelling of the eyelids (allergic conjunctivitis). These symptoms are often associated with exposure to airborne allergens like pollen or pet dander.
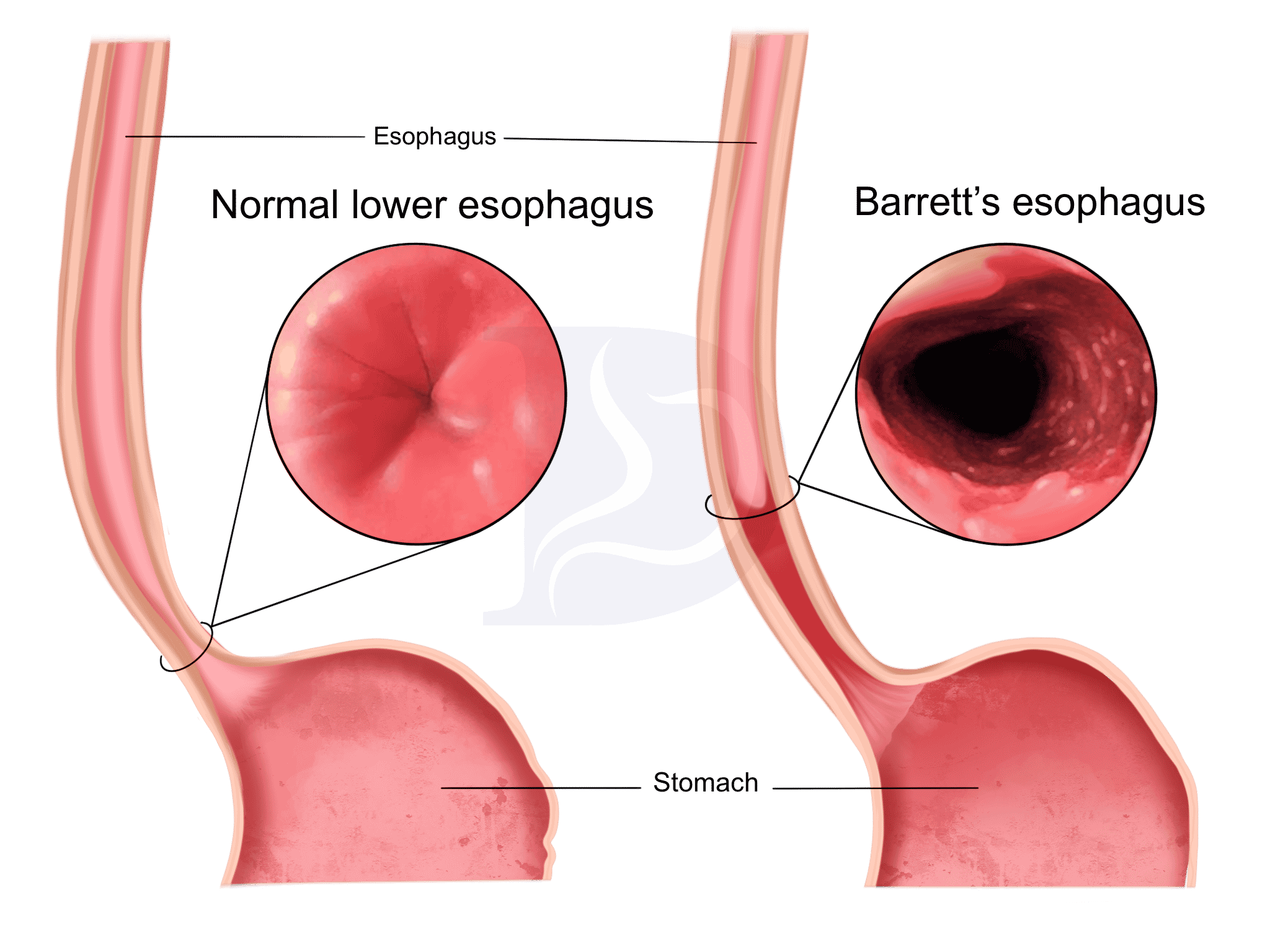
- Gastrointestinal Symptoms: Ingested allergens can trigger gastrointestinal symptoms, including nausea, vomiting, abdominal pain, diarrhea, and in severe cases, anaphylaxis. Food allergies, such as those to peanuts, tree nuts, shellfish, and dairy products, commonly cause these symptoms.
- Systemic Reactions: Severe allergic reactions, known as anaphylaxis, can occur rapidly and affect multiple organ systems. Symptoms may include difficulty breathing, rapid heartbeat, drop in blood pressure, dizziness, loss of consciousness, and swelling of the face, lips, or throat. Anaphylaxis requires immediate medical attention and treatment with epinephrine (adrenaline) to prevent potentially life-threatening complications.
Recognizing and promptly addressing allergic symptoms is essential for effective management and preventing severe complications. (Comprehensive Nursing Paper on Allergies: Understanding, Management, and Education)
Etiology
Pathophysiology
The pathophysiology of allergies involves a complex cascade of immunological events triggered by exposure to allergens. This process leads to the development of allergic reactions, characterized by various symptoms affecting multiple organ systems.
- Sensitization: The initial step in the pathophysiology of allergies is sensitization, wherein the immune system identifies an allergen as a threat and mounts a specific immune response. Upon initial exposure to an allergen, specialized immune cells called antigen-presenting cells (APCs) process and present the allergen to T lymphocytes, activating them.
- IgE Production: Activated T lymphocytes stimulate B lymphocytes to produce immunoglobulin E (IgE) antibodies specific to the allergen. IgE antibodies bind to high-affinity receptors on the surface of mast cells and basophils, sensitizing these cells to subsequent allergen exposure.
- Release of Inflammatory Mediators: Upon re-exposure to the allergen, cross-linking of IgE antibodies on mast cells and basophils triggers the release of inflammatory mediators such as histamine, leukotrienes, and cytokines. These mediators induce vasodilation, increased vascular permeability, smooth muscle contraction, and recruitment of inflammatory cells to the site of allergen exposure.
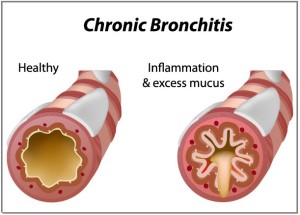
- Inflammatory Response: The release of inflammatory mediators leads to the development of allergic symptoms, affecting various organ systems. In the respiratory system, histamine release causes airway constriction, mucus secretion, and bronchoconstriction, resulting in symptoms like coughing, wheezing, and shortness of breath. In the skin, histamine and other mediators cause itching, redness, and hives. Systemic release of inflammatory mediators can lead to severe allergic reactions known as anaphylaxis, characterized by life-threatening symptoms such as difficulty breathing, drop in blood pressure, and loss of consciousness.
Overall, the pathophysiology of allergies involves a complex immune response triggered by allergen exposure, leading to the development of allergic reactions with various symptoms affecting multiple organ systems. Understanding these underlying mechanisms is crucial for effective allergy management and treatment. (Comprehensive Nursing Paper on Allergies: Understanding, Management, and Education)
DSM-5 Diagnosis
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), does not classify allergies as mental disorders. However, it recognizes the psychological impact of allergies on mental health through associated symptoms such as anxiety and stress.
- Anxiety Disorders: Allergies can exacerbate symptoms of anxiety disorders in susceptible individuals. The fear of experiencing allergic reactions or the anticipation of encountering allergens in specific environments can lead to heightened anxiety levels. For example, individuals with severe food allergies may experience anxiety related to dining out or attending social gatherings where allergens may be present.
- Stress-Related Disorders: Chronic allergies can contribute to stress-related disorders due to their impact on daily functioning and quality of life. Persistent symptoms such as nasal congestion, itching, and fatigue can disrupt sleep patterns, affect concentration, and impair work or school performance. The ongoing management of allergies, including allergen avoidance strategies, medication regimens, and potential allergic reactions, can also contribute to stress levels.
- Psychosomatic Symptoms: Allergies may manifest psychosomatic symptoms, where psychological factors influence physical health. Stress and anxiety associated with allergies can exacerbate existing allergic symptoms or lead to the perception of symptoms in the absence of allergen exposure. For example, heightened stress levels may exacerbate symptoms of allergic rhinitis, leading to increased nasal congestion and discomfort.
While allergies themselves are not classified as mental disorders in the DSM-5, their psychological impact on individuals’ well-being and mental health is recognized. Addressing the psychological aspects of allergies, including anxiety and stress management, can be integral components of comprehensive allergy care and treatment plans. (Comprehensive Nursing Paper on Allergies: Understanding, Management, and Education)


:max_bytes(150000):strip_icc()/hiv-aids-symptoms-4014373-final-ct-003ab16aa2f64faa9209cf4e6a71a555.png)