Nursing Paper Example on Viral Meningitis
Nursing Paper Example on Viral Meningitis
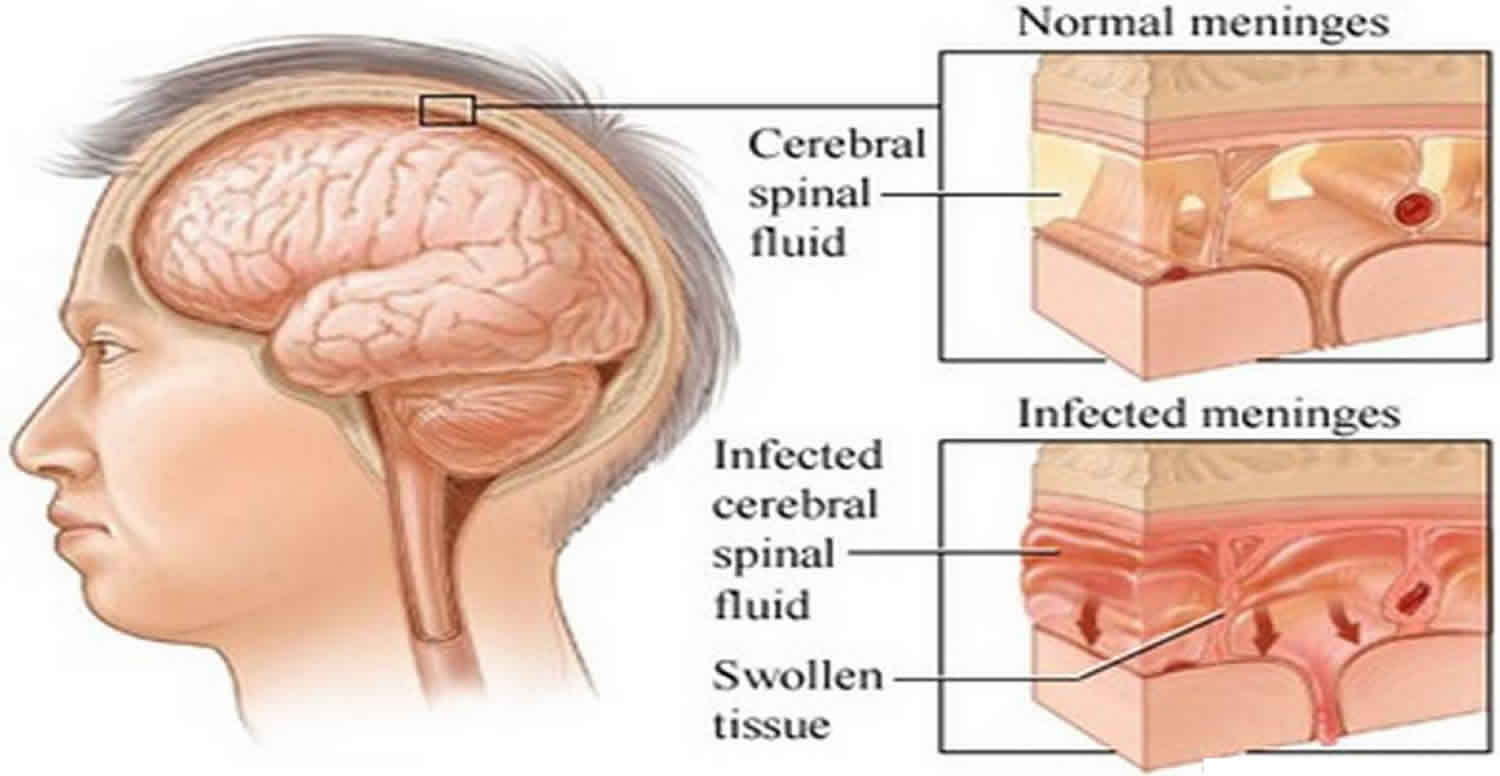
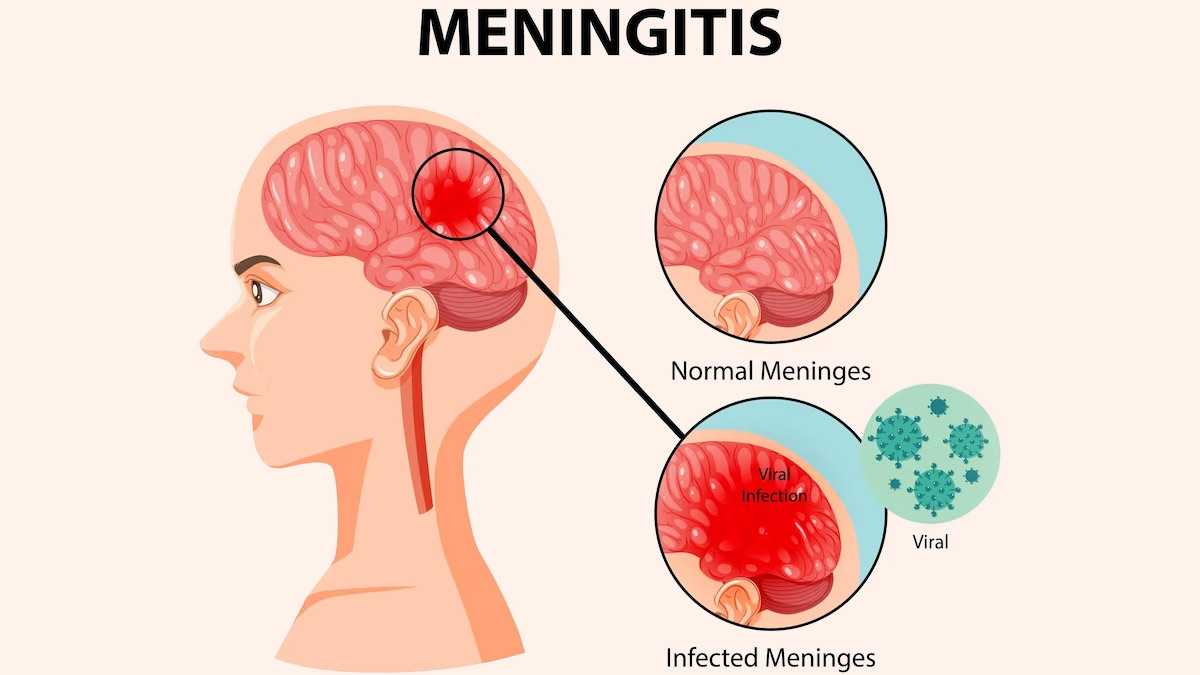
(Nursing Paper Example on Viral Meningitis) Viral meningitis, also known as aseptic meningitis, is an inflammation of the meninges, which are the protective membranes surrounding the brain and spinal cord. Unlike bacterial meningitis, viral meningitis is generally less severe, but it can still cause significant morbidity. This disease is caused by a variety of viruses and can affect people of all ages, though certain populations may be more vulnerable to severe complications.
Causes of Viral Meningitis
Common Viral Causes
The primary causative agents of viral meningitis include:
- Enteroviruses: Responsible for up to 85% of viral meningitis cases, enteroviruses such as Coxsackie and echoviruses are common in late summer and fall.
- Herpes Simplex Virus (HSV): HSV type 2, associated with genital herpes, can cause viral meningitis, particularly in adults.
- Varicella-Zoster Virus (VZV): The virus that causes chickenpox and shingles can also lead to viral meningitis, especially in immunocompromised individuals.
- Mumps Virus: Although rare due to vaccination, mumps can cause viral meningitis in unvaccinated individuals.
- Measles and Influenza Viruses: These viruses are rarer causes of viral meningitis but may still pose a risk, especially in regions with lower vaccination rates.
- Human Immunodeficiency Virus (HIV): In the early stages of infection, HIV can present with meningitis-like symptoms (Centers for Disease Control and Prevention, 2023).
Pathophysiology of Viral Meningitis
Viral meningitis develops when a virus invades the central nervous system, leading to inflammation of the meninges. Once the virus enters the bloodstream, it can cross the blood-brain barrier and reach the central nervous system. The immune system’s response to the viral presence results in the release of cytokines and inflammatory mediators, which cause the classic symptoms of meningitis, including fever, headache, and neck stiffness. Inflammatory processes also increase intracranial pressure, contributing to severe headache and, in some cases, altered mental status (Domingues et al., 2020).
Signs and Symptoms of Viral Meningitis
The clinical presentation of viral meningitis varies by individual, but typical symptoms include:
- Fever: Often low to moderate, though it may be high in some cases.
- Headache: A severe, persistent headache is common, particularly around the temples or behind the eyes.
- Neck Stiffness: Difficulty or pain with neck movement, a classic sign of meningitis.
- Photophobia: Sensitivity to light, often accompanied by eye pain.
- Nausea and Vomiting: These are due to increased intracranial pressure.
- Fatigue and Malaise: Generalized weakness and a lack of energy.
- Altered Mental Status: This may range from mild confusion to lethargy, especially in severe cases (Meningitis Research Foundation, 2021).
Diagnosis of Viral Meningitis
Diagnosing viral meningitis requires differentiating it from other causes of meningitis, particularly bacterial, as treatment and prognosis differ significantly.
Clinical Assessment
The diagnosis begins with a thorough history and physical examination, with attention to pathognomonic symptoms of meningitis, such as neck stiffness, fever, and altered mental status. Recent exposure to viral infections or travel history may provide clues to specific viral causes (Johns Hopkins Medicine, 2022).
(Nursing Paper Example on Viral Meningitis)
Laboratory Tests
- Lumbar Puncture (LP): A lumbar puncture, or spinal tap, is essential for confirming viral meningitis. Cerebrospinal fluid (CSF) analysis in viral meningitis typically shows clear or slightly cloudy fluid, with elevated white blood cell counts (predominantly lymphocytes), normal glucose levels, and normal to slightly elevated protein levels.
- Polymerase Chain Reaction (PCR): PCR testing on CSF is highly sensitive for identifying viral genetic material, especially for enteroviruses, HSV, and VZV.
- Serology: Antibody tests can detect viral-specific IgM or IgG in the blood or CSF, providing indirect evidence of certain viral infections.
- Blood Cultures and Other Tests: Although primarily to rule out bacterial meningitis, blood cultures and additional tests are sometimes conducted to identify other causes or co-infections (Schmidt & Tyler, 2020).
Treatment and Management of Viral Meningitis
Treatment of viral meningitis primarily focuses on supportive care, as most cases resolve without antiviral therapy. However, certain viruses require specific antiviral treatment.
Supportive Care
- Hydration and Electrolyte Management: Adequate hydration is essential, especially in patients experiencing vomiting or decreased oral intake.
- Pain Management: Nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen can relieve fever and headache.
- Rest: Bed rest and reduced activity help the body recover from the infection.
Antiviral Medications
- For Herpes Simplex Virus and Varicella-Zoster Virus: Antiviral drugs such as acyclovir are effective for HSV and VZV and are typically administered intravenously in severe cases.
- For Influenza Virus: Antiviral drugs such as oseltamivir are used if influenza is suspected, especially if the patient is within the first 48 hours of symptom onset.
- For HIV-associated Meningitis: Antiretroviral therapy may be initiated as part of the broader management of HIV (Meningitis Research Foundation, 2021).
Prevention of Viral Meningitis
Preventing viral meningitis involves vaccination, good hygiene, and limiting exposure to individuals with known infections.
Vaccination
- MMR Vaccine: The measles, mumps, and rubella (MMR) vaccine reduces the incidence of meningitis caused by these viruses.
- Varicella Vaccine: Protects against chickenpox and, by extension, VZV-related meningitis.
- Polio Vaccine: Poliovirus, a known cause of viral meningitis, is effectively prevented with the polio vaccine.
Personal Hygiene and Public Health Measures
- Hand Hygiene: Washing hands regularly with soap reduces transmission of enteroviruses and other pathogens.
- Avoiding Contact with Infected Individuals: Limiting contact with individuals displaying symptoms of viral infections reduces the risk of transmission.
- Vector Control: Mosquito control helps prevent viral infections like West Nile virus, which can cause meningitis (Centers for Disease Control and Prevention, 2023).
Prognosis and Complications of Viral Meningitis
The prognosis for viral meningitis is generally favorable, with most patients recovering within 7 to 10 days. However, complications can arise, particularly in certain populations.
Complications
- Seizures: Some patients may experience seizures, especially if the viral infection is severe.
- Chronic Headaches: Persistent headaches are reported in some cases post-recovery.
- Cognitive Impairment: In rare instances, long-term cognitive issues may occur, especially if the central nervous system was extensively affected.
- Recurrent Meningitis: Recurrent episodes are uncommon but may occur with viruses like HSV, particularly in immunocompromised individuals (Domingues et al., 2020).
Conclusion
Viral meningitis is a relatively common and often self-limiting infection of the meninges caused by various viruses. While it generally has a favorable prognosis, timely diagnosis, supportive care, and specific antiviral therapy for certain viruses are essential to minimize complications. Prevention through vaccination and personal hygiene is equally important, particularly in populations at higher risk of severe disease.
References
Centers for Disease Control and Prevention. (2023). Viral meningitis: Causes and prevention. https://www.cdc.gov/meningitis/viral.html
Domingues, R. B., & Tsanaclis, A. M. (2020). Viral meningitis and its long-term effects on the brain. Infectious Disease Clinics of North America, 34(3), 405-421. https://doi.org/10.1016/j.idc.2020.06.004
Johns Hopkins Medicine. (2022). Viral meningitis: Diagnosis and management. https://www.hopkinsmedicine.org/health/conditions-and-diseases/viral-meningitis
Meningitis Research Foundation. (2021). Viral meningitis: Symptoms, causes, and treatments. https://www.meningitis.org