Nursing Paper Example on Rickets
Nursing Paper Example on Rickets
Rickets is a metabolic bone disease that primarily affects children, leading to soft and weakened bones. It results from prolonged deficiency in vitamin D, calcium, or phosphate. These nutrients are crucial for proper bone mineralization and growth, and when they are lacking, bones become soft and malformed. Rickets commonly affects children in developing countries where malnutrition or limited sunlight exposure is prevalent, but cases have also been observed in industrialized nations. Left untreated, rickets can cause severe bone deformities, delayed growth, and other health complications.
Causes
Rickets is mainly caused by a deficiency of vitamin D, which is essential for calcium absorption in the gut. Without adequate vitamin D, the body is unable to maintain proper calcium and phosphate levels, leading to impaired bone mineralization. The primary causes of rickets include:
- Inadequate Vitamin D Intake: Infants and children who are not exposed to sufficient sunlight or whose diets lack vitamin D-rich foods, such as fortified milk, fatty fish, or egg yolks, are at high risk.
- Limited Sunlight Exposure: Vitamin D is synthesized when the skin is exposed to ultraviolet (UV) rays from sunlight. Children who live in regions with limited sunlight or who spend little time outdoors may develop a deficiency.
- Malabsorption Disorders: Conditions like celiac disease, inflammatory bowel disease, or liver disorders can impair the absorption of vitamin D and other essential nutrients.
- Genetic Forms of Rickets: Rare inherited disorders, such as hypophosphatemic rickets or vitamin D-dependent rickets, affect how the body processes or responds to vitamin D or phosphate, leading to bone weakening.
Signs and Symptoms
The symptoms of rickets usually manifest during periods of rapid growth, such as infancy or early childhood. Common signs and symptoms include:
- Bone Pain and Tenderness: Children may complain of aching bones, especially in the legs, pelvis, or spine.
- Skeletal Deformities: Soft bones can lead to visible deformities such as bowed legs, knock knees, or a pigeon chest (protruding breastbone).
- Delayed Growth: Children with rickets often experience stunted growth or delayed motor milestones, such as walking.
- Dental Problems: Poor bone mineralization can affect tooth development, leading to dental defects, delayed eruption, or increased susceptibility to cavities.
- Muscle Weakness: Muscle tone may be reduced, causing difficulty with movements or delayed motor skills.
- Hypocalcemia (Low Calcium Levels): Severe cases can lead to low blood calcium levels, which may result in muscle cramps, seizures, or difficulty breathing.
If left untreated, these symptoms may become more severe, causing permanent bone deformities and increasing the risk of fractures.
(Nursing Paper Example on Rickets)
Etiology
Rickets is primarily caused by insufficient levels of vitamin D, which impairs calcium and phosphate absorption. This deficiency can result from:
- Nutritional Deficiency: Diets lacking in vitamin D-rich foods, or those with insufficient exposure to fortified products, can lead to rickets. Breastfed infants who do not receive vitamin D supplements may be at higher risk, as breast milk contains low levels of vitamin D.
- Sunlight Deprivation: Children who are not exposed to adequate sunlight, either due to cultural practices, living in regions with long winters, or excessive use of sunscreen, can develop vitamin D deficiency.
- Malabsorption Disorders: Conditions like Crohn’s disease, cystic fibrosis, and celiac disease interfere with nutrient absorption, including vitamin D, calcium, and phosphate, leading to rickets.
- Renal Disease: Kidney disorders can affect the body’s ability to activate vitamin D or maintain proper phosphate levels, contributing to rickets.
Pathophysiology
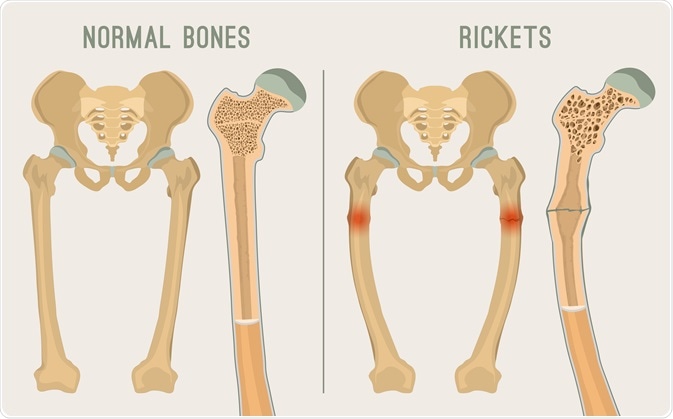
In normal bone formation, vitamin D facilitates the absorption of calcium and phosphate from the intestines, which are then used for mineralization of the bone matrix. In rickets, vitamin D deficiency or impaired metabolism disrupts this process, leading to decreased calcium and phosphate levels in the blood. As a result, the bones become soft and less able to withstand pressure, leading to the characteristic skeletal deformities. In the absence of adequate mineralization, growth plates (the areas of growing tissue near the ends of long bones) remain soft, contributing to bowed legs or knock knees as the child grows.
Diagnosis
Rickets is diagnosed based on a combination of clinical presentation, radiological findings, and laboratory tests. The diagnostic process includes:
- Physical Examination: A healthcare provider will look for signs of skeletal deformities, delayed growth, and muscle weakness.
- Blood Tests: These are done to measure levels of calcium, phosphate, and vitamin D. In rickets, calcium and phosphate levels may be low, while alkaline phosphatase (an enzyme linked to bone activity) is elevated.
- X-rays: Radiographic imaging is crucial for diagnosing rickets. X-rays of the wrists, knees, or long bones may show widened growth plates, bone softening, and fractures.
- Bone Biopsy: In rare cases, a bone biopsy may be performed to assess bone structure and mineralization directly.
(Nursing Paper Example on Rickets)
Treatment Regimens
The treatment of rickets aims to correct the underlying nutritional deficiency and support proper bone development. Treatment options include:
- Vitamin D Supplementation: High-dose vitamin D therapy is essential to correct the deficiency and prevent further complications. Vitamin D3 (cholecalciferol) is typically administered either orally or through injections in severe cases.
- Calcium and Phosphate Supplementation: Oral calcium supplements are given to support bone mineralization, particularly if dietary intake is inadequate. In cases of hypophosphatemic rickets, phosphate supplements may be necessary.
- Dietary Adjustments: Increasing the intake of vitamin D-rich foods (e.g., fatty fish, fortified milk, and egg yolks) and calcium-rich foods (e.g., dairy products, leafy green vegetables) is recommended to promote bone health.
- Sunlight Exposure: Encouraging children to spend more time outdoors in the sun can help stimulate natural vitamin D production.
- Treatment of Underlying Disorders: In cases of rickets due to malabsorption or genetic conditions, treating the primary disorder is crucial to improving vitamin D and calcium metabolism.
Prevention
Preventing rickets requires ensuring adequate intake of vitamin D, calcium, and phosphate during periods of rapid growth. Key prevention strategies include:
- Vitamin D Supplementation: Infants, especially those who are exclusively breastfed, should receive vitamin D supplements as recommended by healthcare providers.
- Sunlight Exposure: Ensuring that children spend sufficient time outdoors in natural sunlight can help prevent vitamin D deficiency. However, it is important to balance sunlight exposure with skin cancer prevention measures.
- Balanced Diet: A diet rich in vitamin D and calcium is essential for growing children. This can be achieved through fortified foods, dairy products, or supplements if necessary.
Complications
Untreated rickets can lead to several serious health complications, including:
- Permanent Bone Deformities: Severe rickets can cause irreversible skeletal deformities, such as bowed legs or a deformed chest.
- Fractures: The weakened bones are more susceptible to fractures.
- Delayed Development: Children with rickets may experience delayed motor development, stunted growth, and muscle weakness.
- Dental Problems: Poor bone mineralization can lead to dental issues, including malformed teeth, increased cavities, and delayed tooth eruption.
(Nursing Paper Example on Rickets)
Patient Education
Educating families and communities about the importance of vitamin D and calcium intake is essential in preventing rickets. Key educational points include:
- Vitamin D-Rich Diet: Emphasizing the importance of including foods rich in vitamin D and calcium in a child’s diet.
- Safe Sunlight Exposure: Encouraging safe outdoor play and limited use of sunscreen to ensure adequate vitamin D production while still preventing sunburn.
- Supplementation: Ensuring that children, especially those at high risk of deficiency, receive appropriate vitamin D supplements as recommended by healthcare professionals.
Conclusion
Rickets remains a preventable and treatable condition, yet it continues to affect children worldwide, particularly in regions where malnutrition and limited access to healthcare are prevalent. By addressing the nutritional deficiencies underlying the disease, promoting awareness of adequate sunlight exposure, and ensuring proper dietary intake, healthcare professionals can help reduce the global burden of rickets. Early intervention is essential to prevent long-term complications, such as bone deformities and delayed growth.
(Nursing Paper Example on Rickets)
References
- Mayo Clinic. Rickets. https://www.mayoclinic.org/diseases-conditions/rickets/symptoms-causes/syc-20351983
- National Health Service (NHS). Rickets. https://www.nhs.uk/conditions/rickets/
- Thacher, T. D., & Fischer, P. R. (2013). “Vitamin D–Deficiency Rickets in Developing Countries.” The New England Journal of Medicine, 369(21), 2044-2055. https://doi.org/10.1056/NEJMra1305361
- World Health Organization (WHO). Vitamin D Deficiency. https://www.who.int/nutrition/topics/vitamind/en/
- Holick, M. F. (2006). “High Prevalence of Vitamin D Inadequacy and Implications for Health.” Mayo Clinic Proceedings, 81(3), 353-373. https://doi.org/10.4065/81.3.353

